CHAPTER 15
Asymmetries, Transverse Deviations, and Forced Bites
Asymmetries
Asymmetry in the dentition can be caused by a difference between the left and right sides in terms of facial skeletal configuration or position of teeth within the jaws or by a combination of both. Small asymmetries of the skull and face, as well as misalignment of the midlines of the dental arches, occur frequently and are rarely troublesome.1–3 Asymmetries in facial configuration can be traced to genetic factors, trauma, or pathologic processes. Deviating facial growth can cause and/or exacerbate asymmetries. Asymmetries in tooth position may be caused by differences in the location where corresponding teeth are formed, premature loss or extraction of deciduous teeth followed by migration, or agenesis or extraction of permanent teeth.
Angle added subdivisions to his classification to account for asymmetries. A Class II subdivision has distoclusion on one side and neutroclusion on the other side. An analogous condition exists in a Class III subdivision, in which mesioclusion is present on one side and neutroclusion on the other side. According to Angle, it is not possible to have distoclusion on one side and mesioclusion on the other side.4
Asymmetries in the occlusion caused by the facial skeletal configuration are usually caused by a deviation in the mandible (Fig 15-1). There are various types of asymmetries caused by deviant locations of tooth formation sites6,7 (Fig 15-2).
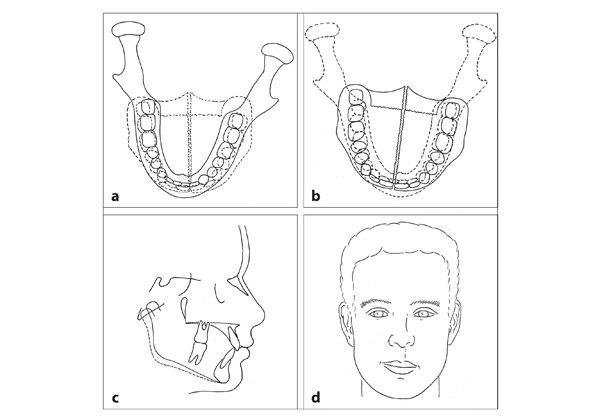
Fig 15-1 Asymmetry in facial configuration. In most humans, the facial skeleton is slightly asymmetric.5 Also, muscles and other soft tissues often differ between the left and right sides. The mandible can be positioned asymmetrically because the locations of the temporal fossae do not correspond. (a) In addition, the mandible itself can be asymmetric. (b) Asymmetry of the face and the maxilla is usually associated with some asymmetry of the mandible. (c) In asymmetry of the lower part of the face, both the size and the shape of the two sides of the mandible are usually different. (d) A small asymmetry in the face is not noticed; a large one is. The positions of the teeth adjust to the asymmetry of the facial skeleton. The dentoalveolar compensatory mechanism plays an essential role in this adjustment.
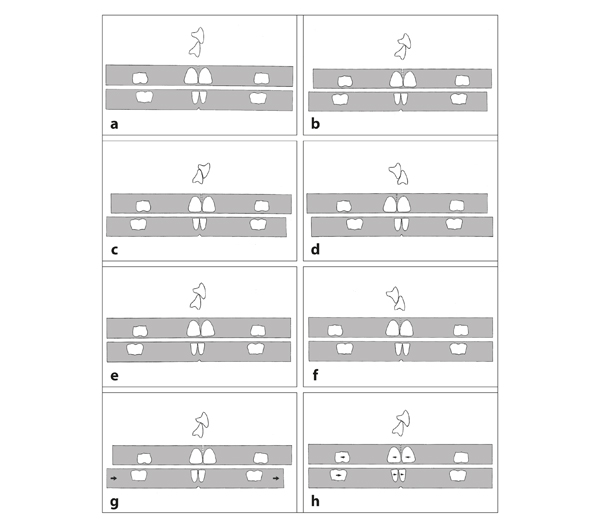
Fig 15-2 Asymmetry in occlusion. (a) Schematic presentation of an ideal situation. An asymmetry in jaw size or position can lead to deviations in the occlusion, such as a Class II, division 1 subdivision (b), a Class II, division 2 subdivision (c), or a Class III subdivision (d). The midlines of the two dental arches also can deviate without asymmetry of the jaws or the posterior occlusion. Such an asymmetry can result from a deviating position of the mandibular or maxillary anterior teeth or from a combination of both. If the molars are also positioned asymmetrically, a Class II subdivision (e) or a Class III subdivision (f) will result. (g) The asymmetry can also be caused by an anomaly in the mandible and result in a Class II subdivision. (h) Asymmetries in the dental arches may simply be the result of abnormal tooth positions.
As indicated, asymmetry in the dental arches can arise secondary to or become aggravated by premature loss of deciduous teeth (Fig 15-3) and agenesis or extraction of permanent teeth. This occurs because teeth tend to migrate in the direction where a tooth is missing (Fig 15-4).
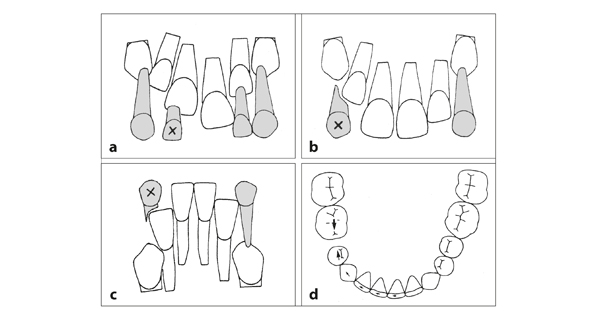
Fig 15-3 Asymmetry after premature loss of deciduous teeth. Premature loss of deciduous anterior teeth is usually a sign of crowding. (a) A maxillary lateral deciduous incisor may resorb when the central permanent incisor erupts. (b) A deciduous canine may resorb when the lateral permanent incisor erupts. (c) The latter occurs more often in the mandible than in the maxilla.8 (d) Premature loss of deciduous molars—mostly due to tooth decay—can lead to tooth migration and result in asymmetry of the occlusion.
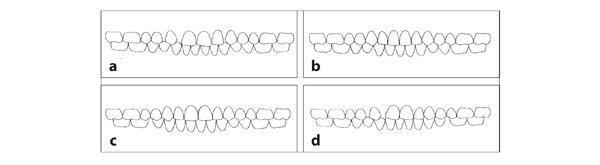
Fig 15-4 Asymmetry due to agenesis or extraction of a permanent tooth. (a) A missing maxillary right lateral permanent incisor will result in tipping of the other three incisors to the right side, but the roots will not pass the median suture. (b) However, there is no structure in the mandible that prevents the migration of an incisor through the median plane. (c) Agenesis of a mandibular second premolar leads to migration on both sides. (d) Agenesis of a maxillary right lateral permanent incisor and of a mandibular left second premolar has a cumulative effect on the deviation of the midlines of the dental arches.
Transverse Deviations
There is a large variation in asymmetries and transverse deviations of the dentition in children and adults. Differences between the left side and the right side in sagittal occlusion of the posterior region (ie, subdivisions) are associated with deviations of the midlines of the dental arches (Figs 15-5 to 15-7). Sometimes the transverse occlusion deviates only on one side (Fig 15-8). The transverse occlusion can also deviate on both sides, as in a telescoping bite, ie, complete maxillary buccal crossbite (Figs 15-9 and


