Chapter 13
Sexually Transmitted Diseases
Sexually transmitted diseases (STDs) continue to be a major health problem worldwide and, in many instances, are on the increase. In the United States, some of the highest rates of infection occur in adolescents and young adults. More than 25 STDs have been identified and are listed in < ?xml:namespace prefix = "mbp" />
TABLE 13-1 Sexually Transmitted Diseases
| Disease | Pathogen |
|---|---|
| Acquired immunodeficiency syndrome (AIDS) | Human immunodeficiency virus (HIV) |
| Amebiasis | Entamoeba histolytica |
| Bacterial vaginosis | Bacteroides spp., Mobiluncus spp. |
| Chancroid | Haemophilus ducreyi |
| Condyloma acuminatum (genital warts) | Human papillomavirus (HPV-6, HPV-11) |
| Cytomegalovirus infection | Cytomegalovirus |
| Enterobiasis | Enterobius vermicularis |
| Epididymitis, mucopurulent cervicitis, lymphogranuloma venereum, nongonococcal urethritis, pelvic inflammatory disease, Reiter’s syndrome | Chlamydia trachomatis |
| Epididymitis, gonorrhea, mucopurulent cervicitis, pelvic inflammatory disease | Neisseria gonorrhoeae |
| Genital herpes | Herpes simplex viruses (HSV-1, HSV-2) |
| Giardiasis | Giardia lamblia |
| Granuloma inguinale (donovanosis) | Calymmatobacterium granulomatis |
| Hepatitis B | Hepatitis B virus (HBV) |
| Molluscum contagiosum | Poxvirus |
| Nongonococcal urethritis, nonspecific vaginitis | Trichomonas vaginalis |
| Nongonococcal urethritis | Ureaplasma urealyticum |
| Pediculosis | Pediculus pubis |
| Salmonellosis | Salmonella spp. |
| Shigellosis | Shigella spp. |
| Streptococcal infection | Group B streptococci |
| Syphilis | Treponema pallidum |
| Vulvovaginal candidiasis | Candida spp., Torulopsis spp. |
STDs have important implications for clinical practice in dentistry:
• STDs are transmitted by intimate interpersonal contact, which can result in oral manifestations. Dental health professionals need to be cognizant of these manifestations as a basis for referral of patients for proper medical treatment.
• Some STDs can be transmitted by direct contact with lesions, blood, or saliva, and because many affected persons may be asymptomatic, the dentist should approach all patients as though disease transmission were possible and must adhere to standard precautions.
• A single STD is accompanied by additional STDs in about 10% of cases, and STD-associated genital ulceration increases the risk for human immunodeficiency virus (HIV) infection.
• Pathogens responsible for STDs can exhibit antimicrobial resistance, thus proper treatment is essential.
• Some STDs are incurable, but all are preventable.
• Patient interaction with dental health care workers can be an important component of STD control by providing opportunities for diagnosis, education, and information regarding access to treatment.
Although most STDs have the potential for oral infection and transmission, discussion in this chapter is limited to gonorrhea, syphilis, and select human herpesvirus and human papillomavirus infections, because these entities are of special interest or importance in the provision of dental care and serve to illustrate basic principles.
Gonorrhea
Definition
Gonorrhea is an STD of worldwide distribution that is caused by Neisseria gonorrhoeae. It produces symptoms in men that usually cause them to seek treatment soon enough to prevent serious sequelae, but maybe not soon enough to prevent transmission to others. Infections in women often do not produce recognizable symptoms until complications have emerged. Because gonococcal infections among women frequently are asymptomatic, an important component of gonorrhea control in the United States continues to be the screening of women who are at high risk for STDs. Of note, patients infected with N. gonorrhoeae often are coinfected with Chlamydia trachomatis.
Epidemiology
Incidence and Prevalence
Gonorrhea is the second most commonly reported infectious disease and STD in the United States, behind chlamydial infection. An estimated 700,000 new cases are reported each year in the United States, and about half of these are reported to the Centers for Disease Control and Prevention (CDC).
Humans are the only natural hosts for this disease, and its occurrence is worldwide. Gonorrhea is transmitted almost exclusively by sexual contact, whether genital–genital, oral–genital, or rectal–genital. The primary sites of infection are the genitalia, the anal canal, and the pharynx.
Gonorrhea can occur at any age, although it is seen most commonly in sexually active teenagers and young adults (8.5 per 1000 in the 15- to 29-year-old age group) and in the South. Rates of infection are similar in men and women, but differ by racial background. African Americans and Hispanics have 20.5 times higher rates of gonorrhea than whites.
Etiology
Gonorrhea is caused by N. gonorrhoeae, a gram-negative intracellular diplococcus. N. gonorrhoeae is an aerobic microbe that replicates easily in warm, moist areas and preferentially requires high humidity and specific temperature and pH for optimum growth. It is a fragile bacterium that is readily killed by drying, so it is not easily transmitted by fomites. It develops resistance to antibiotics rather easily, and many strains have become resistant to penicillin, tetracycline, and quinolones.
Pathophysiology and Complications
N. gonorrhoeae infects columnar epithelium (as found in the mucosal lining of the urethra and cervix) and transitional epithelium (as in the oropharynx and rectum), whereas stratified squamous epithelium (skin and mucosal lining of the oral cavity) generally is resistant to infection.
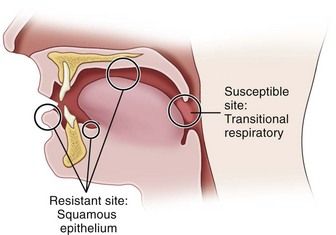
FIGURE 13-1 Areas of relative epithelial susceptibility to infection by Neisseria gonorrhoeae within the oral cavity.
Infection in men usually begins in the anterior urethra. The bacteria invade epithelial tissues and are engulfed within polymorphonuclear leukocytes, leading to cytokine production and purulent discharge.
Infection in women occurs most commonly in the cervix and the urethra. Invasion of cervical epithelium can be associated with the production of a purulent exudate but more often leads to an ascending infection of the endometrium, fallopian tubes, ovaries, and pelvic peritoneum. The ascending infection is a common cause of pelvic inflammatory disease (PID), which affects about 1 million women each year in the United States.
In both genders, gonorrhea of the rectum may occur after anal–genital intercourse or through direct anal contamination from genital lesions. Infection of the pharynx and oral cavity is predominantly seen in women and homosexual men after fellatio. It also occasionally is seen after cunnilingus.
Widespread dissemination is more likely in infected persons lacking select complement proteins. The gonococcemia can lead to variety of disorders, including migratory arthritis, skin and mucous membrane lesions, endocarditis, meningitis, PID, and pericarditis.
Clinical Presentation
Signs and Symptoms
In men, symptoms usually occur after an incubation period of 2 to 5 days, although they may take as long as 30 days to appear. The most common findings include a mucopurulent (white, yellow, or green) urethral discharge, burning pain on urination, urgency, and frequency. Tenderness and swelling of the meatus may occur.
In women, a significant percentage of cases may be asymptomatic or only minimally symptomatic. Symptomatic infection may demonstrate vaginal or urethral discharge, dysuria with frequency and urgency, and burning pain when urinating. Backache and abdominal pain also may be present.
Approximately 50% of women and 1% to 3% of men are asymptomatic or only mildly symptomatic. This is unfortunate because patients may not seek medical care for their problem and as a result constitute a large reservoir of infection.
Gonococcal infection of the anal canal commonly is less intense than genital infection, but similar signs and symptoms, including a copious purulent discharge, soreness, and pain, may be noted.
Within the oral cavity, the pharynx is most commonly affected.
Gonococcal stomatitis or oral gonorrhea is uncommon; case reports in the literature are limited.
Laboratory Findings
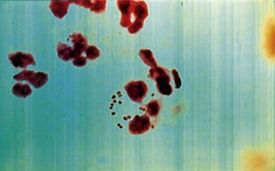
Laboratory diagnosis of a genital N. gonorrhoeae infection can be made based on the finding of gram-negative diplococci within polymorphonuclear leukocytes in a smear of urine or of purulent discharge in symptomatic mean (
Medical Management
The CDC recommendations
The clinician should be aware that gonococcal pharyngitis is more difficult to eradicate than infections at urogenital and anorectal sites.
Syphilis
Definition
Syphilis is an acute and chronic STD, caused by Treponema pallidum, that produces skin and mucous membrane lesions in the acute phase and bone, visceral, cardiovascular, and neurologic disease in the chronic phase. The variety of systemic manifestations associated with the later stages of syphilis resulted in its historical designation as the “great imitator” disease. As with gonorrhea, humans are the only known natural hosts for syphilis. The primary site of syphilitic infection is the genitalia, although primary lesions also occur extragenitally. Syphilis remains an important infection in contemporary medicine because of the morbidity it causes, and because it enhances the transmission of HIV.
Epidemiology
Incidence and Prevalence
Syphilis is the fifth most frequently reported STD in the United States today, surpassed only by chlamydial infection, gonorrhea, salmonellosis, and AIDS. In 1990, the incidence of primary and secondary syphilis reached 50,223 cases.
Congenital syphilis occurs when the fetus is infected in utero by an infected mother. In 2008, a total of 431 cases of congenital syphilis were reported to the CDC. This represents a rate of 10.1 per 100,000 live births—higher than the 8.2 cases per 100,000 live births in 2005—but still a dramatic decline from the peak of 107.3 cases per 100,000 live births in 1991.
Etiology
The etiologic agent of syphilis is Treponema pallidum, which is a slender, fragile anaerobic spirochete. It is transmitted predominantly sexually, including by oral–genital and rectal–genital contact with contaminated sores. However, transmission also can occur through nonsexual means such as kissing, blood transfusion, or accidental inoculation with a contaminated needle. Indirect transmission by fomites is possible but uncommon, because the organism survives for only a short time outside the body.
Pathophysiology
Available evidence suggests that T. pallidum does not invade completely intact skin; however, it can invade intact mucosal epithelium and gain entry through minute abrasions or at the hair follicles. Within a few hours after invasion, bacterial spread to the lymphatics and the bloodstream occurs, resulting in early widespread dissemination of the disease. The early response to bacterial invasion consists of endarteritis and periarteritis.
Clinical Presentation
Signs and Symptoms
Manifestations and descriptions of syphilis are classically divided according to stages of the disease, with each stage having its own specific signs and symptoms related to disease duration and antigen-antibody responses. The stages are primary, secondary, latent, tertiary, and congenital. Of note, many infected persons do not develop symptoms for years, yet remain at risk for late complications if the infection is not treated.
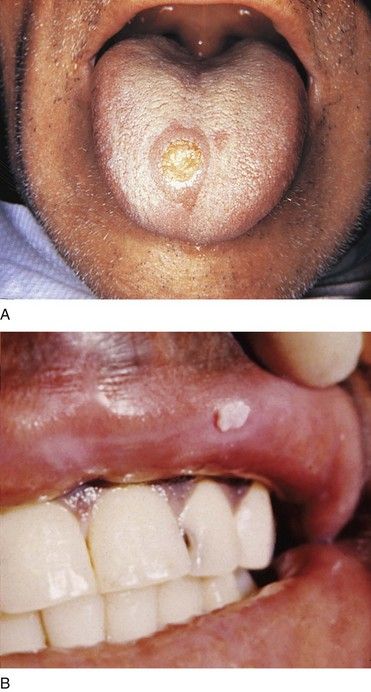
Primary Syphilis
The classic manifestation of primary syphilis is the chancre, a solitary firm, round, granulomatous lesion that develops at the site of inoculation with the infectious organism. The chancre usually occurs within 2 to 3 weeks (range, 10 to 90 days) after exposure (

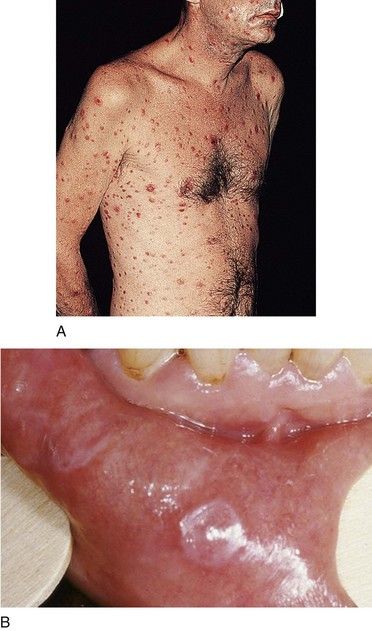
Secondary Syphilis
The manifestations of secondary syphilis appear 6 to 8 weeks after initial exposure. The chancre may or may not have completely resolved by this time. The symptoms and signs of secondary syphilis include fever, arthralgia and malaise, generalized lymphadenopathy, and patchy hair loss and develop in 80% of patients. Generalized eruptions of the skin and mucous membranes also occur (
Latent Syphilis
Latent syphilis is defined as an untreated infection in which the patient displays seroreactivity but no clinical evidence of disease. This stage of the infection is divided into early latent syphilis (disease acquired within the preceding year) and late latent syphilis (disease present for longer than 1 year) or latent syphilis of unknown duration. During the first 4 years of latent syphilis, patients may exhibit mucocutaneous relapses and are considered infectious. After 4 years, relapses do not occur, and patients are considered noninfectious (except for blood transfusions and pregnant women).
Tertiary (Late) Syphilis
The tertiary (late) stage occurs in roughly 1/3 of untreated persons, generally several years after disease onset.
More than 80% of manifestations of tertiary syphilis are essentially vascular in nature and result from an obliterative endarteritis. Cardiovascular syphilis most commonly manifests as an aneurysm of the ascending aorta.
The benign tertiary stage of syphilis is classically characterized by the formation of gummas. These localized nodular, tender lesions may involve the skin, mucous membranes, bone, nervous tissue, and/or viscera. They are thought to be the end result of a delayed hypersensitivity reaction. Pathologically, they consist of an inflammatory granulomatous lesion with a central zone of necrosis. Gummas are not infectious but can be destructive.
The oral lesions of tertiary syphilis consist of diffuse interstitial glossitis and the gumma. Interstitial glossitis should be considered a premalignant condition. The tongue may appear lobulated and fissured with atrophic papillae, resulting in a bald-appearing and wrinkled surface. Leukoplakia frequently is present. The oral gumma is a rare lesion that most commonly involves the tongue and palate. It appears as a firm tissue mass with central necrosis. Palatal gummas may perforate into the nasal cavity or maxillary sinus.
Neurosyphilis can occur during any stage of syphilis. It can produce a meningitis-like syndrome, Argyll Robertson pupils (which react to accommodation but not to light), altered tendon reflexes, general paresis, tabes dorsalis (degeneration of dorsal columns of the spinal cord and sensory nerve trunks), difficulty in coordinating muscle movements, cognitive dysfunction or insanity.
Congenital Syphilis
Syphilis or its sequelae occur in the newborn if the mother is infected while carrying the child. The disease is transmitted to the fetus in utero, usually after the 16th week, because before this time, the placenta prevents transmission of bacteria. The disease persists worldwide because a substantial number of women do not receive serologic testing for syphilis during pregnancy, or they may undergo testing too late in pregnancy to receive prenatal care.

Laboratory Findings
T. pallidum has never been cultured successfully on any type of medium; therefore, the definitive diagnosis of syphilis is made from a positive darkfield microscopic examination or on the basis of direct immunofluorescent antibody tests on fresh lesion exudates. Darkfield examination yields consistently positive findings only during primary and early secondary stages. Definitive diagnosis of oral lesions by this method is difficult, because other species of Treponema are indigenous to the oral cavity.
Syphilis typically is diagnosed by a two-step process involving a nonspecific (screening) antibody test, followed by a treponeme-specific test. Screening antibody tests of blood also are known as serologic tests for syphilis (STS). These tests are of two basic types, indirect and direct, and are differentiated by the types of antibodies they measure.
Screening Serologic Tests for Syphilis: Nontreponemal Tests—VDRL and RPR
Standard screening tests for syphilis consist of the Venereal Disease Research Laboratory (VDRL) slide test, the rapid plasma reagin (RPR) test, and the automated reagin test (ART). These indirect, nontreponemal serologic tests are designed to detect the presence of an antibody-like substance called reagin that is produced when T. pallidum reacts with various body tissues. They are equally valid. A disadvantage of reaginic tests is the occasional biologic false-positive result that can occur.
Nontreponemal tests produce titers (reported quantitatively as serologic dilutions [e.g., 1 : 2, 1 : 4, 1 : 8]) that usually correlate with disease activity. Results are consistently positive and the highest titers are obtained between 3 and 8 weeks after the appearance of the primary chancre. In primary syphilis, nontreponemal tests usually revert to negative within 12 months after successful treatment. In secondary syphilis, up to 24 months may be required for the patient to become seronegative. Occasionally, a patient will remain seropositive for life, or will test positive in the presence of an associated infection or condition (false-positive). With tertiary syphilis, many patients remain seropositive fo/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


