The Dynamics of Change
 Outline
OutlinePhysical Changes
Body
Figure 12-1 shows the difference in the proportions of the fetus at 2 and 5 months, the newborn’s body, and the changes that are made during maturation. No year is more dramatic in terms of growth than the first year of life, during which most children undergo a 50% increase in length and almost a 200% increase in weight. Toward the end of the first year of life, the growth rate slows. After the first birthday, the growth rate stays very stable and the height and weight increments of the child remain relatively predictable all the way to adolescence.
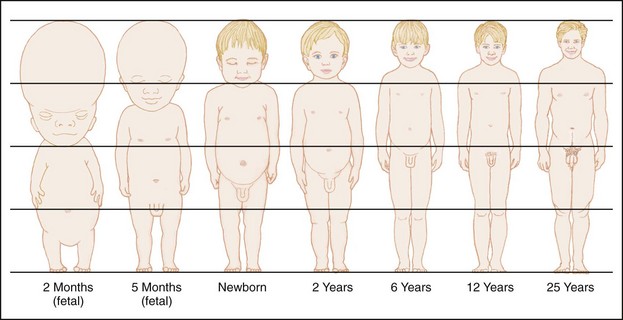
 FIGURE 12-1
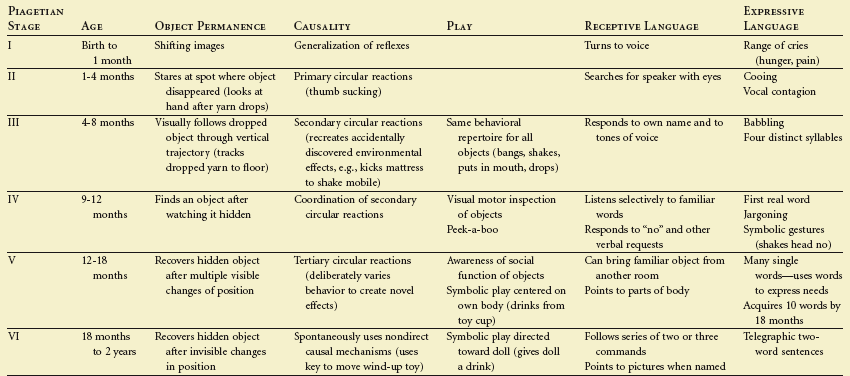
FIGURE 12-1As the body changes and matures, the infant is afforded increasingly sophisticated postural and locomotive actions. Table 12-1 shows some of the physical and cognitive developmental hallmarks of a child during his or her first 18 months of life. (Piagetian psychology as well as object permanency and causality is discussed in this chapter’s section on cognitive development.)
 TABLE 12-1
TABLE 12-1
From Zuckerman BS, Frank DA: In Levine MD, Carey WB, Crocker AT et al, editors: Developmental-behavioral pediatrics, Philadelphia, 1983, Saunders, p 91.
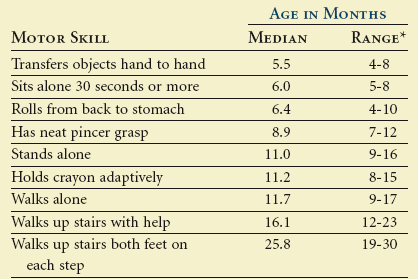
By age 2 years, a child has the gross motor skills to run, climb, walk up and down steps, and kick a ball. His fine motor skills allow him to stack blocks (up to six), make parallel crayon strokes, and turn the pages of a book one page at a time. Table 12-2 shows a variety of motor skills and the mean age at which they are acquired.
 TABLE 12-2
TABLE 12-2
Median Age and Range in Acquisition of Motor Skills
Adapted from Bayley N: Manual for the Bayley scales of infant development, New York, 1969, Psychological Corporation. From Zuckerman BS, Frank DA: Infancy. In Levine MD, Carey WB, Crocker AT et al, editors: Developmental-behavioral pediatrics, Philadelphia, 1983, Saunders.
The nervous system of the child grows dramatically from birth until age 3 years. In fact, by the end of the second year the child’s brain has attained 75% of its adult weight.1
Craniofacial Changes
Intrauterine Growth and Development
The organization and complexity of growth and development are nowhere more evident than in the changes that take place in the head and face (Table 12-3). The human face begins its first observable growth during the fourth week of intrauterine life with the development of the branchial apparatus. The branchial apparatus is first seen as a series of ridges on the lateral aspect of the cephalic end of the embryo at approximately the third week of intrauterine life. A 1-month-old embryo has no real face but the key primordia have already begun to gather. These slight swellings, depressions, and thickenings then rapidly undergo a series of mergers, rearrangements, and enlargements that transform them from a cluster of separate masses into a face (Figure 12-2).2
 TABLE 12-3
TABLE 12-3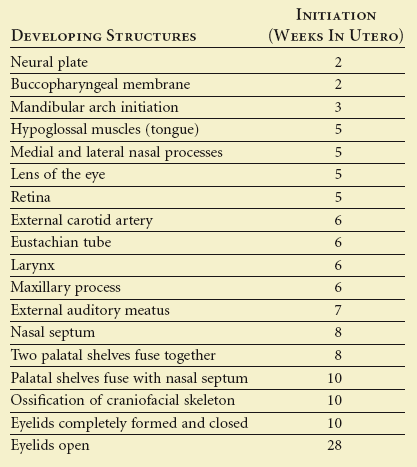
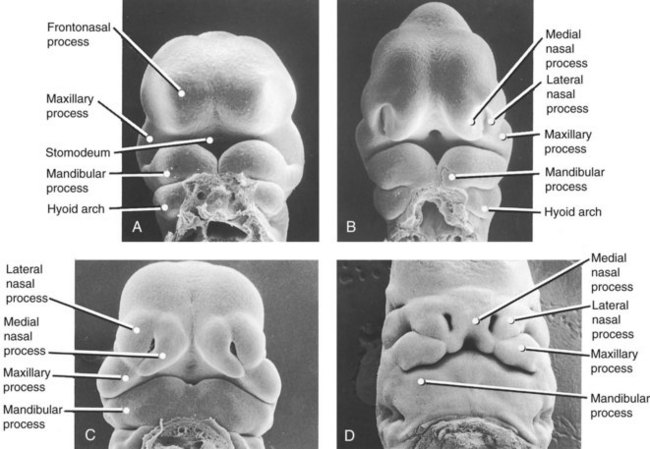
 FIGURE 12-2
FIGURE 12-2Sperber3 described the presomite stage of development (21 to 31 days), during which the 3-mm embryo develops at its cranial end five mesenchymal elevations or processes. The five mesenchymal elevations constitute the initial features of the face. These include the frontonasal process, two maxillary processes, and two mandibular arches. These processes grow differentially, and by obliterating the ectodermal grooves between them, they eventually contour the features of the face.
The oral cavity of the embryo is bounded by the frontonasal process and by the maxillary and mandibular processes of the first branchial arch (Figure 12-3). Each maxillary process moves toward the midline and joins with the lateral nasal fold of the frontonasal process. As this is happening, a shelflike process (the palatal process) develops on the medial side of each maxillary process. These two palatal processes move toward the midline, where they fuse. This palatal fusion is normally completed by the eighth intrauterine week. The mandibular processes fuse at the midline somewhat before the maxillary and nasal processes (Figure 12-4). The palate grows more rapidly in width than in length during the fetal period as a result of midpalatal sutural growth and appositional growth of the lateral alveolar margins. A failure in the fusion of the processes gives rise to oral or facial clefts or both. In the mandible, the cartilaginous skeleton of the first branchial arch, known as Meckel cartilage, provides a form for the development of the mandible.

 FIGURE 12-3
FIGURE 12-3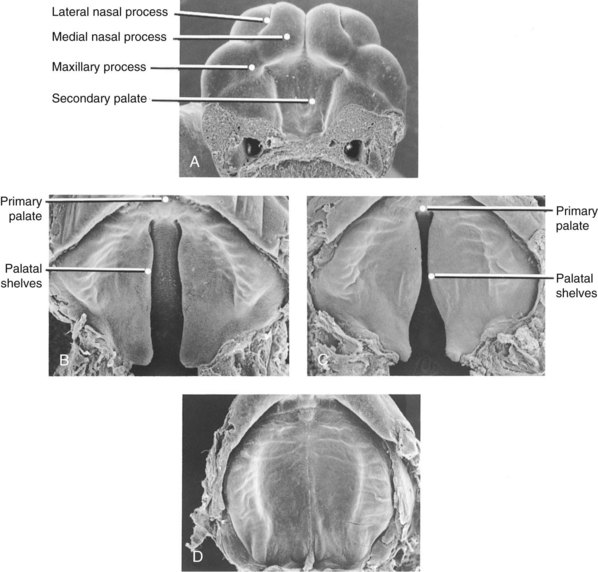
 FIGURE 12-4
FIGURE 12-4The growth of the nasoseptal region contributes to frontomaxillary, frontonasal, frontozygomatic, and zygomaticomaxillary sutured changes. The expansion of the eyeballs, the brain, and the sphenooccipital synchondrosal cartilage also acts in separating the facial sutures. The overall effect of these diverse forces of expansion is osseous buildup on the posterior surface of the facial bones.4
Unlike the embryonic period, during the fetal period the size of the maxilla relative to the mandible varies widely. Throughout the embryonic stage, the mandible is considerably larger than the maxilla. It is not until the fetal stage that the maxilla is more developed than the mandible. Subsequent to this, the mandible grows at a greater pace and equals the size of the maxilla by 11 weeks in utero. Between the 13th and the 20th weeks in utero, mandibular growth again lags relative to the maxilla. At birth, the mandible tends to be retrognathic to the maxilla.5 During the remainder of its intrauterine existence the fetus undergoes a process of growth and maturation and a reorganization of the spatial relationships among various structures.6
The major remodeling of the early facial skeleton that occurs throughout the remainder of the fetal period begins in the fetus at about 14 weeks. Before this time, the bones enlarge in all directions from their respective ossification centers. Remodeling, a process that accompanies growth, starts when the definitive form of each of the individual bones of the face and cranium is attained (Figure 12-5).6
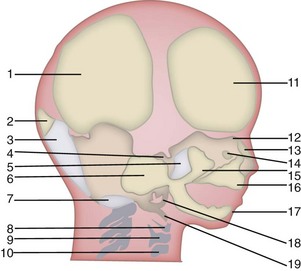
 FIGURE 12-5
FIGURE 12-5 weeks). 12, Crista galli (still cartilaginous; inferiorly, the middle concha begins ossification at 16 weeks, the superior and inferior conchae at 18 weeks; the perpendicular plate of ethmoid begins ossification during the first postnatal year, the cribriform plate during the second postnatal year, the vomer at 8 fetal weeks). 13, Nasal bone (8 weeks). 14, Lacrimal bone (
weeks). 12, Crista galli (still cartilaginous; inferiorly, the middle concha begins ossification at 16 weeks, the superior and inferior conchae at 18 weeks; the perpendicular plate of ethmoid begins ossification during the first postnatal year, the cribriform plate during the second postnatal year, the vomer at 8 fetal weeks). 13, Nasal bone (8 weeks). 14, Lacrimal bone ( weeks). 15, Malar (8 weeks). 16, Maxilla (end of sixth week; premaxilla, 7 weeks). 17, Mandible (6 to 8 weeks). 18, Tympanic ring (begins at 9 weeks, with complete ring at 12 weeks; petrous bone, 5 to 6 months). 19, Styloid process, still cartilaginous.
weeks). 15, Malar (8 weeks). 16, Maxilla (end of sixth week; premaxilla, 7 weeks). 17, Mandible (6 to 8 weeks). 18, Tympanic ring (begins at 9 weeks, with complete ring at 12 weeks; petrous bone, 5 to 6 months). 19, Styloid process, still cartilaginous. Growth and Development after Birth
At birth, the bony face and skull show little differentiation from child to child. Newborns have tiny mouths and virtually no chins. Their faces are small, although their eyes, in comparison with the small face, are exceedingly large. The forehead and top of the head are big. It is difficult to imagine the diversity of individual looks that will develop over the course of childhood and adolescence from such similar infant faces (Figure 12-6).

 FIGURE 12-6
FIGURE 12-6At birth, the maxilla is very low frontally and relatively small. By 9 months, the jaw has become considerably wider and higher. There is also a remarkable increase in the maxillary sinus. At birth, the bones that compose the cranium are not fused and are separated by six membrane-filled gaps called fontanels (Figure 12-7). Each of these areas is completely closed by ossification within 2 years of birth.
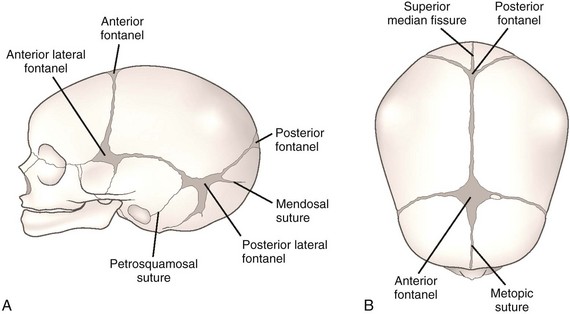
 FIGURE 12-7
FIGURE 12-7The face appears broad and flat at birth. The lower jaw seems underdeveloped and receded. The overall broadness of the face results from the lack of vertical growth, which is still to come. The horizontal dimensions are more nearly adultlike. The upper and total face heights are not even half completed at birth. According to Ranly,7 they are 43% and 40%, respectively, which means that the most striking and complex growth of the head is associated with the face. After an initial spurt during the first 3 years, the rate of increase of these dimensions slows. It remains steady until the adult size is reached. The cranium, as represented by cranial width and length, is closer to adult size than any other part of the head. This can be explained by the development of the brain, which by the eighth month of intrauterine life has all of the nerve cells it will ever have. The growth of the cranial vault is complete before that of the maxilla, and maxillary growth is complete before mandibular growth. This is an example of the cephalocaudal growth gradient, which indicates that the cranial structures are closer to their adult size during infancy and childhood than other body parts.8 Symphyseal growth increases the width of the mandible. By the second year, the symphysis is closed and growth becomes localized in the mandible as well as in the nasomaxillary complex. An enormous metamorphosis has taken place, but many more changes need to occur before the child’s adult appearance is realized.
Dental Changes
The 6-week-old fetus demonstrates 10 sites of epithelial activity on the occlusal (soft tissue) border of both the developing maxilla and the mandible.9 These sites are lined up next to each other and ultimately predict the position of the future 10 primary teeth in both the maxilla and the mandible (Figure 12-8).
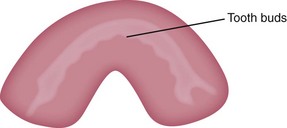
 FIGURE 12-8
FIGURE 12-8In addition to developing 20 primary teeth, each unit also develops a dental lamina that is responsible for the development of the future permanent tooth.9 Therefore, the primary centrals, laterals, and cuspids produce a dental lamina for the future permanent centrals, laterals, and cuspids. The first and second primary molars produce a dental lamina for the future first and second permanent premolars. The unaccounted-for permanent molars develop from and on three successive locations on one dental lamina extending distally from each of the second primary molars (Figure 12-9).9
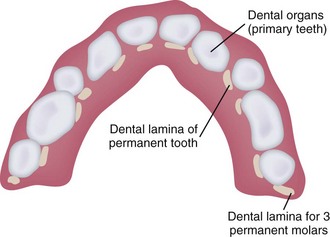
 FIGURE 12-9
FIGURE 12-9An analysis of the successive periods of growth of the tooth germ can be organized by the following stages of the life cycle of the tooth9:
Growth
Initiation
The initiation stage is first noticed in the 6-week-old fetus (Figure 12-10). As the word initiation suggests, this stage is recognized by the initial formation of an expansion of the basal layer of the oral cavity immediately above the basement membrane. The basal layer is a row of organized cells lined up on the basement membrane, which is a tissue division line between the ectoderm (epithelium) and the mesoderm (Figure 12-11). The cells of the basal layer are the innermost cells of the oral epithelium (ectoderm) adjacent to the basement membrane.
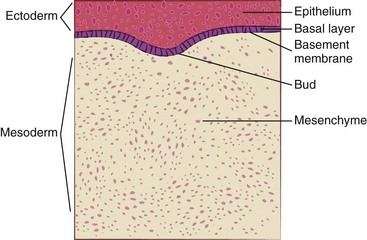
 FIGURE 12-10 The initiation stage of the life cycle of the tooth in an approximately 5- to 6-week-old fetus.
FIGURE 12-10 The initiation stage of the life cycle of the tooth in an approximately 5- to 6-week-old fetus.
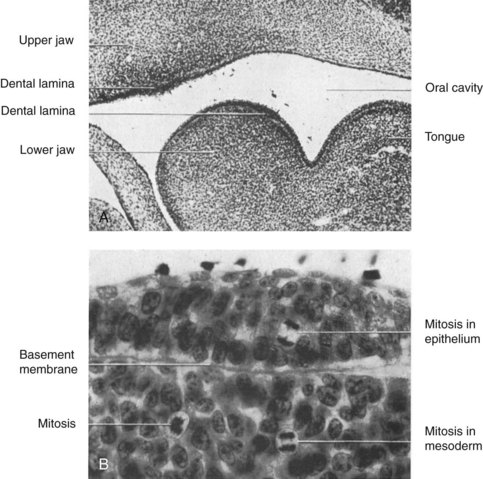
 FIGURE 12-11
FIGURE 12-11At 10 specific intermittent locations along the basement membrane, the cells of the basal layer multiply at a much faster rate than the surrounding cells.10 This development occurs at that point on the oral epithelium that is the tooth bud and is responsible for the initial growth of that tooth (Figure 12-12).
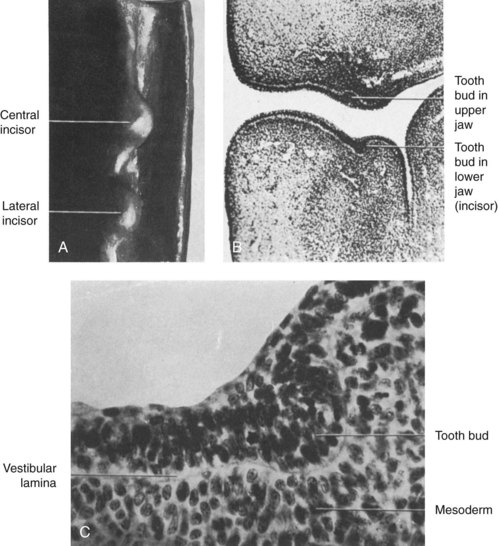
 FIGURE 12-12
FIGURE 12-12It can be noted that the times of initiation of the various teeth differ.11 This period of tooth development is also recognized as the bud stage. Such a description assists in visually understanding the developmental process of the immature tooth.
Proliferation
Proliferation is really only a further multiplication of the cells of the initiation stage and an expansion of the tooth bud, resulting in the formation of the tooth germ (Figure 12-13). The tooth germ is a result of the prolific epithelial cells forming a caplike appearance with the subsequent incorporation of the mesoderm. This incorporation of mesodermal tissue below and within the cap gives rise to the dental papilla.
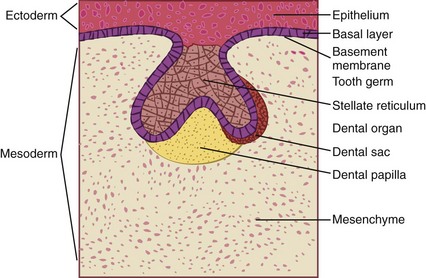
 FIGURE 12-13 The proliferation stage of the life cycle of the tooth in an approximately 9- to 11-week-old fetus.
FIGURE 12-13 The proliferation stage of the life cycle of the tooth in an approximately 9- to 11-week-old fetus.
As the tooth germ continues to proliferate in an irregular fashion, it produces a caplike appearance. This stage is called the cap stage because the structure takes on the form of a cap (Figure 12-14). Like the bud stage, it is so referenced for visual identification. As the cap begins to form, the mesenchyme changes within the cap to initiate the development of the dental papilla.
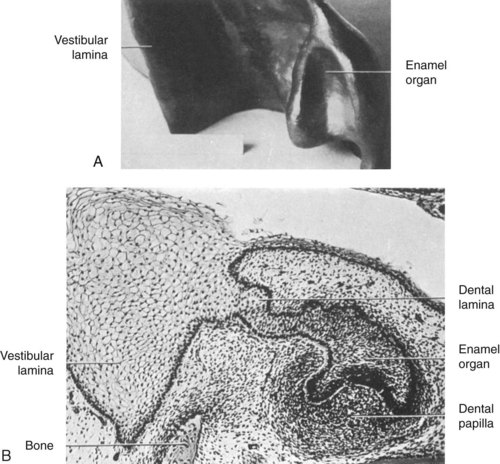
 FIGURE 12-14
FIGURE 12-14The dental papilla evolves from the mesenchyme invaginating the inner dental epithelium and specializes to form the pulp and dentin. The dental sac also comes into being by a marginal condensation in the mesenchyme surrounding the dental organ and dental papilla. The stellate (starlike) reticulum (network) is an organization of cells within the descending portion of the dental organ that is enamel-forming tissue and is called the enamel pulp. Therefore the tooth germ during this stage has all the necessary formative tissues to embrace the development of a tooth and its periodontal ligament.9
In summary, the tooth germ consists of all the necessary elements for the development of the complete tooth. The germ is composed of the following three distinct parts: (1) dental organ, (2) dental papilla, and (3) dental sac. The dental organ produces the enamel. The dental papilla generates the dentin and pulp. The dental sac gives rise to the cementum and periodontal ligament.9
Histodifferentiation
The histodifferentiation stage is marked by the histologic difference in the appearance of the cells of the tooth germ because they are now beginning to specialize (Figure 12-15). The cap continues to grow and begins to look more like a bell. The image of a bell is registered because the extensions of the cap grow deeper into the mesoderm. This part of development is appropriately called the bell stage, and the tissue within the bell gives rise to the dental papilla.
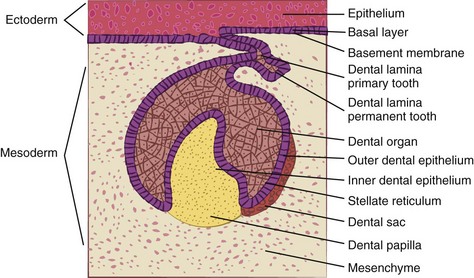
 FIGURE 12-15 The histodifferentiation stage of the life cycle of the tooth. Approximately 14-week-old fetus.
FIGURE 12-15 The histodifferentiation stage of the life cycle of the tooth. Approximately 14-week-old fetus.
The dental lamina continues to shrink with the result that it looks more like a cord. The dental lamina for the permanent successor becomes obvious as an extension of the dental lamina of the primary tooth. The basal layer continues to exist and is now divided into an inner and an outer dental epithelium. The stellate reticulum expands and organizes to incorporate more intercellular fluid in preparation for the formation of enamel (Figures 12-16 to 12-18).
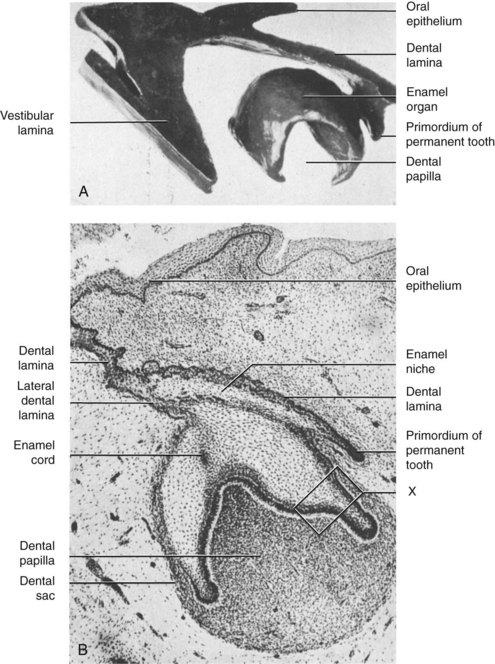
 FIGURE 12-16 Bell stage of tooth development. Human embryo 105 mm long, 14th week. A, Wax reconstruction of lower central incisor. B, Labiolingual section of the same tooth. X designates inset (see Figure 12-17). (From Orban B: Dental histology and embryology, ed 2, New York, 1929, McGraw-Hill.)
FIGURE 12-16 Bell stage of tooth development. Human embryo 105 mm long, 14th week. A, Wax reconstruction of lower central incisor. B, Labiolingual section of the same tooth. X designates inset (see Figure 12-17). (From Orban B: Dental histology and embryology, ed 2, New York, 1929, McGraw-Hill.)
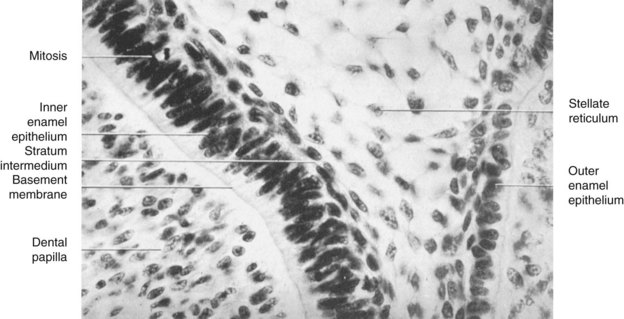
 FIGURE 12-17 The four layers of the epithelial dental organ in high magnification (area “X” of Figure 12-16). (From Orban B: Dental histology and embryology,
FIGURE 12-17 The four layers of the epithelial dental organ in high magnification (area “X” of Figure 12-16). (From Orban B: Dental histology and embryology,
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


