CHAPTER 11
Sandwich Osteotomy Bone Graft in the Anterior Mandible
You can observe a lot just by watching.
—Yogi Berra
Almost any grafting procedure for the thin, atrophic, relatively avascular anterior mandible has led to complications. Block grafts tend to dehisce or not consolidate, guided bone regeneration techniques fail to provide sufficient gains in width and height, and alveolar distraction osteogenesis is often too complicated or too risky to perform for a small segment. On the other hand, the use of the anterior mandibular sandwich osteotomy has been observed to have a much lower complication rate in the treatment of significant vertical defects.
Vertical alveolar augmentation of the anterior mandible is accomplished relatively easily with a sandwich osteotomy bone graft technique.1 Unlike in the maxilla, in the mandible, tension from the lingual soft tissue pedicle does not greatly inhibit repositioning of the elevated alveolus to the ideal alveolar plane as the alveolar crest is placed at the same time in an axially appropriate position. 2 Osteotomy segments can sometimes be moved 10 mm or more vertically; however, most movements are 4 to 8 mm.3 Vertical overcorrection can also be done, which allows subsequent removal of a thin alveolar crest at the time of implant placement.
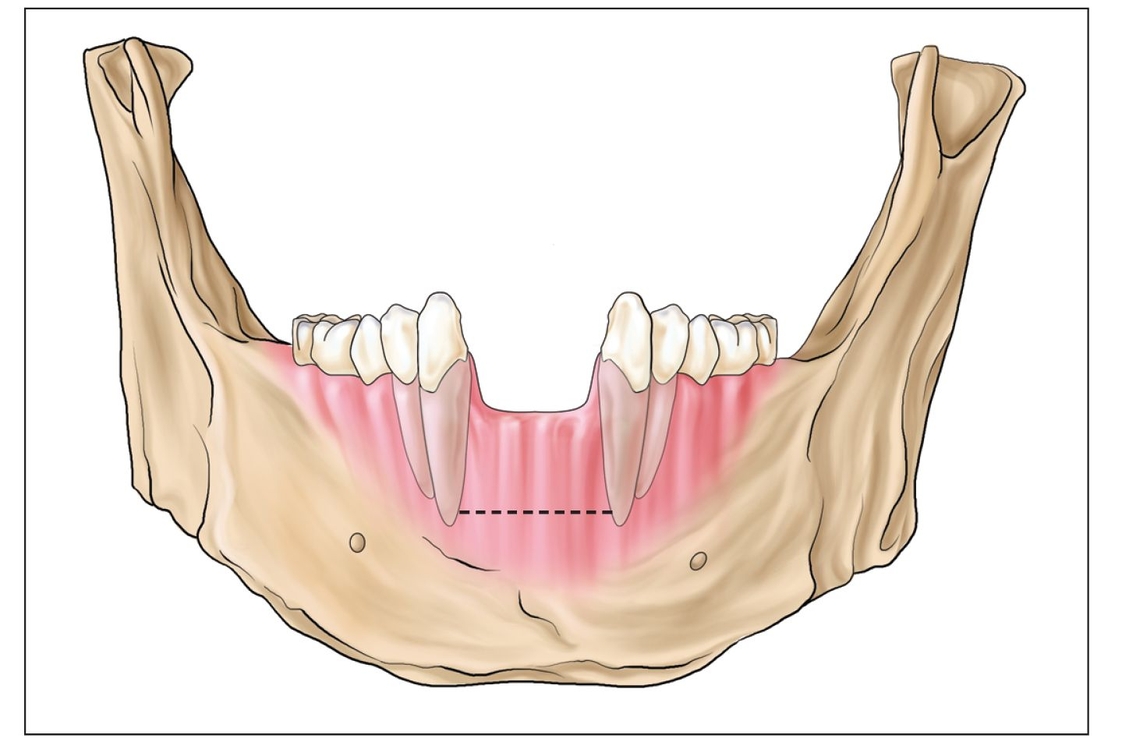
Fig 11-1a The anterior mandible is approached through a vestibular incision (dotted line) for the sandwich osteotomy.
The anterior mandible is a special situation in which the loss of vertical height due to periodontal disease often leaves a significant vertical defect that is highly amenable to treatment with the sandwich osteotomy. Anterior mandibular teeth are within the esthetic zone, and the gingival margin may sometimes be observed on facial expression. 4 Although most patients do not display the alveolar zone of the anterior mandible, when the zone is visible, the same surgical and esthetic criteria for maxillary anterior sandwich osteotomy apply to the mandible.5
A typical anterior mandibular setting is one in which the incisors are missing but the canines remain, although they most likely appear elongated because of periodontal disease. Failure to recognize this factor can lead to esthetic compromise because of the reduced canine bone level, even if a sandwich osteotomy is properly executed. The segment can generally only be advanced crestally as far as the bone level at the adjacent teeth.
 Case Selection
Case Selection
Although mandibular implants are almost always easily placed without augmentation grafting, prosthetic restoration of the alveolus is often required. When gingival display is present and profile emergence from gingival tissue is desirable, the sandwich osteotomy is an excellent option for treatment. This will help avoid the need for a fixed hybrid prosthesis.
The osteotomy procedure requires a basal bone width of 4 or 5 mm. If, however, vertical resorption is severe and extends to the genial tubercle, a segmental osteotomy is probably contraindicated.6
Fig 11-1b Vertical cuts are made 2 mm from adjacent tooth roots and then connected with a horizontal osteotomy.
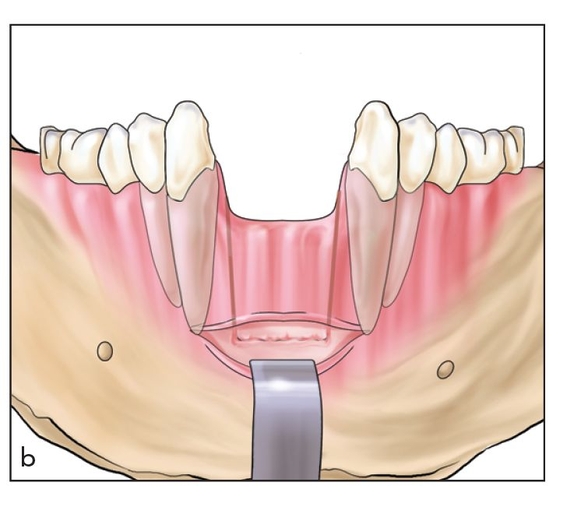
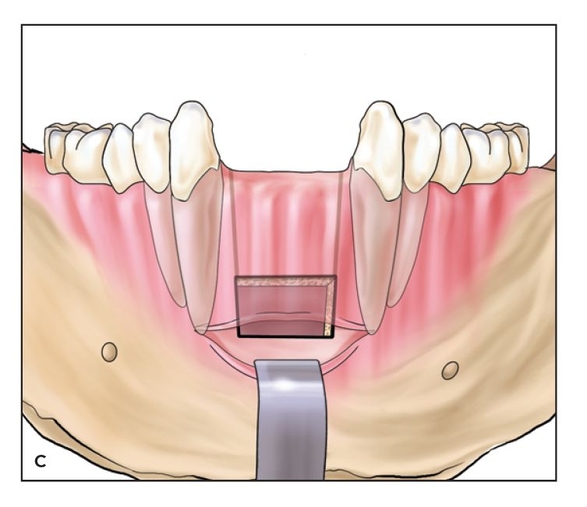
Fig 11-1c The segment is freed with an osteotome and elevated, ideally to the alveolar plane. When bone is lost from adjacent root surfaces, elevation is limited to the vertical height of bone at the adjacent teeth.
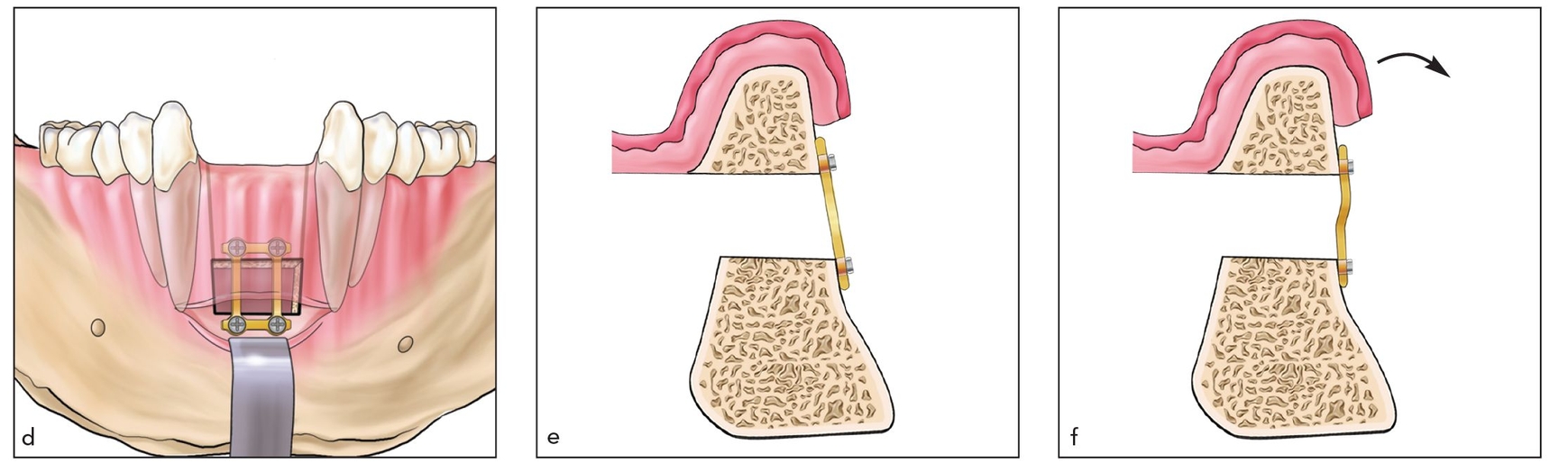
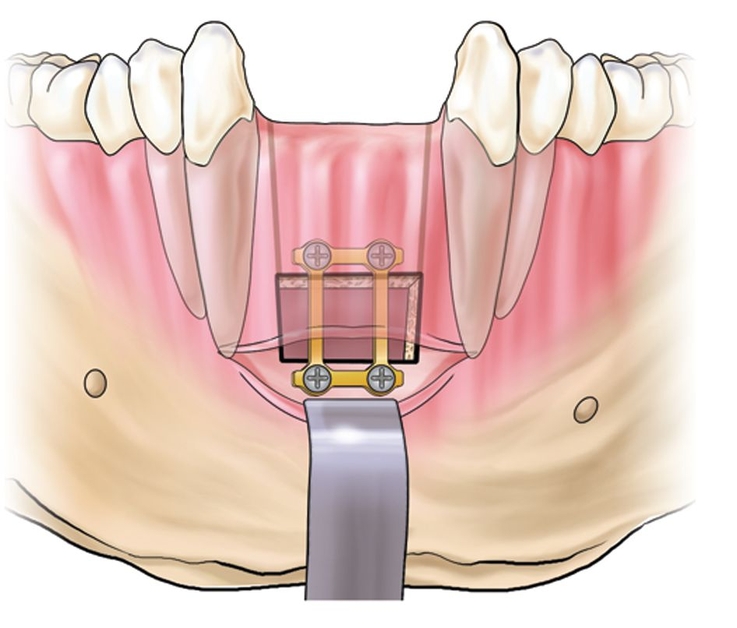
Figs 11-1d to 11-1f The segment is fixed with a bone plate (or a block inlay graft). A wire twister can then be used to torque (arrow) the segment into axial alignment.
 Surgical Technique
Surgical Technique
In the anterior mandible the surgeon must be aware of the mental foramina, often located near the apex of the first premolar roots.7 If canines are included in the proposed osteotomy, the nerve must be avoided during exposure of the site and protected during the osteotomy procedure. The segment must also be of adequate width or, if narrow crestally, must have adequate bone at the base to allow the horizontal cut.
The mentalis muscle attachment, if high, is important to consider in order to avoid chin ptosis. A vestibular incision is made at the depth of the vestibule, usually about 5 mm below the attached gingival tissue8 (Fig 11-1a). Reflection of a mucoperiosteal flap is avoided toward the alveolar crest, and inferior reflection should avoid complete detachment of the mentalis muscle.
A horizontal osteotomy cut is made through this wound with an oscillating saw; the osteotomy is made carefully to avoid injury to the lingual mucoperiosteum.9 Vertical cuts are made just adjacent to the canines or between the canine and first premolar if the canines are included in the osteotomy (Fig 11-1b). When teeth are included in the osteotomy, vertical movement is usually limited to about 5 mm; edentulous areas can be moved 8 to 10 mm vertically. Vertical osteotomies near teeth should leave 2 mm of bone next to the root surface.10
Following completion of the osteotomy, the segment is moved until it is level with the ideal alveolar plane or level with the height of bone at the adjacent teeth11 (Fig 11-1c). The segment is then fixed with a small bone plate and grafted interpositionally (Fig 11-1d). After fixation, the plate is used to carefully torque the segment forward into axial alignment (Figs 11-1e and 11-1f). The wound is closed primarily without tension (Figs 11-1g and 11-1h).
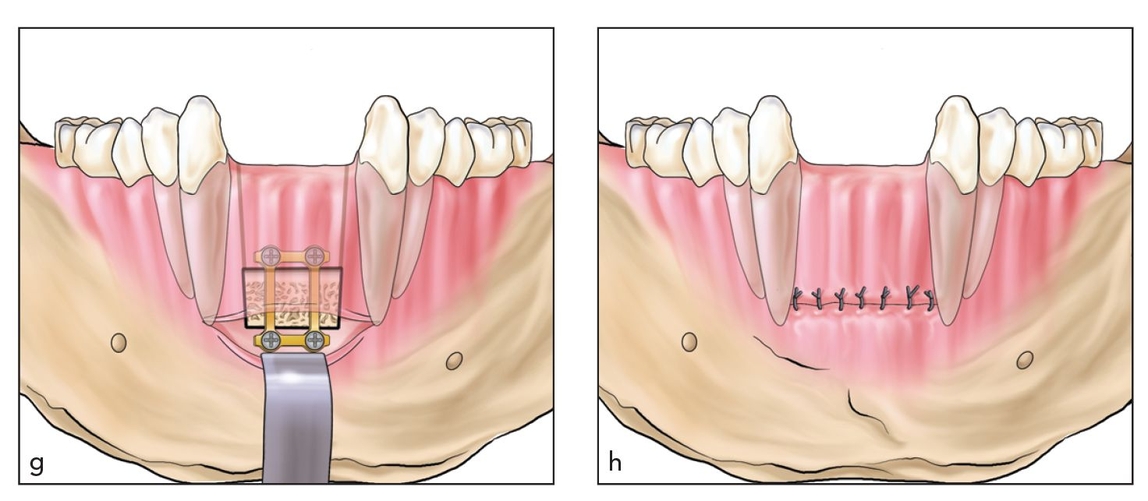
Figs 11-1g and 11-1h The wound is closed primarily after grafting.
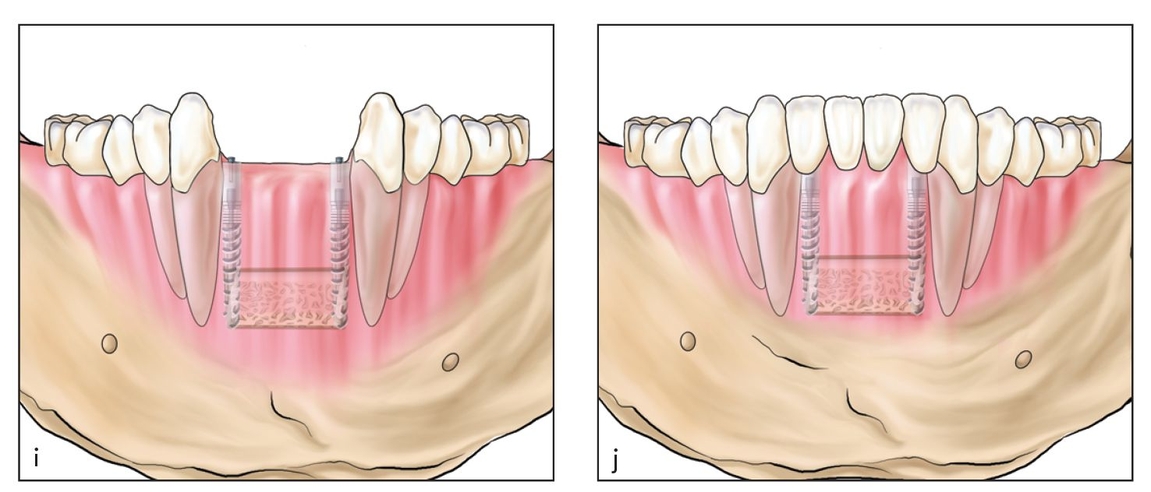
Figs 11-1i and 11-1j Implants are subsequently placed and restored. Implants should extend in length beyond the interpositional graft site to ensure primary stability.
Implants are placed 4 months after the osteotomy, and the prosthesis is placed 4 months after the implants (Figs 11-1i and 11-1j).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


