CHAPTER 11
Class II, Division 1 Malocclusion
A malocclusion is usually not a pathologic condition but rather a disharmonious combination of variables in the dentition and face that on their own do not exceed the normal range of variation. Individuals with a malocclusion are not sick, have no pain, and mostly do not experience physical discomfort.1 The term malocclusion literally indicates that the occlusion is bad.
Angle Classification of Malocclusion
In 1899, Edward H. Angle introduced a classification to create order among the large diversity of malocclusions. The Angle classification is based on, and limited to, the occlusion and is purely descriptive. The term occlusion refers to the relationship between mandibular and maxillary teeth in functional contact.2 The Angle classification only considers the sagittal aspect of the occlusion. Other aspects, such as open and deep bites, are not included. Despite its limitations, the Angle classification is generally accepted and used worldwide.
A normal sagittal relationship of the dental arches (ie, neutroclusion) is called Class I. If the position of the mandibular dental arch is too posterior in relation to the maxillary dental arch (ie, distoclusion), it is called a Class II malocclusion. If the reverse situation exists—the mandibular dental arch is too far anterior in relation to the maxillary dental arch (ie, mesioclusion)—it is called a Class III malocclusion. The terms Class II and Class III do not indicate whether the abnormality lies in the mandible or the maxilla or in both. In fact, nothing is suggested regarding the cause of the malocclusion.
In addition, Angle categorized the Class II malocclusions as either Class II, division 1 or Class II, division 2. In Class II, division 1 malocclusions, the maxillary incisors are inclined normally or too far labially. In Class II, division 2 malocclusions, to be discussed in the next chapter, two or more maxillary incisors are palatally inclined. In severe Class II, division 1 malocclusions, the lower lip is positioned between the mandibular and maxillary incisors. In Class II, division 2 malocclusions, the lips are closed.
Malocclusions in which the sagittal occlusion differs between the left and right sides were named subdivisions by Angle. A Class II subdivision means that a normal occlusion (ie, neutroclusion) exists on one side and a distoclusion on the other side. The Class II subdivision is discussed in chapter 15 together with the Class III subdivision. This chapter also does not cover the deviations in the dental arches that can complicate a Class II, division 1 malocclusion. However, it is important to understand that all of the abnormalities mentioned in chapter 10 can occur in Class II, division 1; Class II, division 2; and Class III malocclusions.
Characteristics of Class II, Division 1 Malocclusions
It also holds true in Class II malocclusions that the mandible cannot grow further in the transverse plane after 6 months of age, while the maxilla can. The rule that the mandibular dental arch serves as a mold for the transverse positioning of the maxillary posterior teeth also applies to Class II malocclusions.
For this discussion of the development of Class II, division 1 malocclusions, it is assumed that no abnormalities were initially present in the dental arches. Rather, deviations developed secondary to the distoclusion.
Because the mandibular dental arch position is too posterior in relation to the maxillary dental arch, the latter will have a smaller width than normal. This results in the permanent dentition being housed in a narrower and sometimes more tapering maxillary dental arch. This is not a primary aspect of the Class II, division 1 malocclusion but a secondary effect of the distoclusion.
A comparable phenomenon occurs in the anterior region. Due to the distoclusion, the permanent incisors will not end up in normal, reciprocally supported contact. The mandibular and maxillary incisors will continue to erupt until they are slowed down and stopped by the occlusal contact, lip, tongue, or palate. This results in an enlarged overjet and overbite. Furthermore, the overeruption of the mandibular anterior teeth leads to a deepening of the curve of Spee (Figs 11-1 to 11-9). Note that many illustrations in this chapter are based on a distoclusion of one premolar crown width; however, most Class II, division 1 malocclusions show distoclusion of one-third to two-thirds of a premolar crown width.
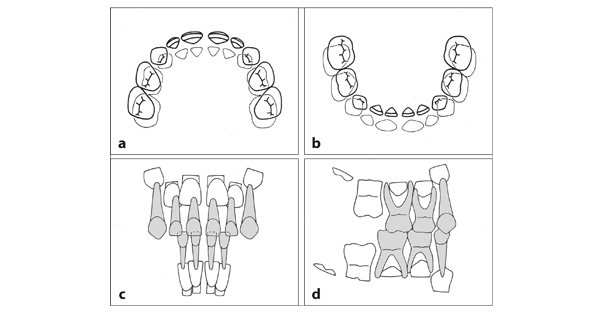
Fig 11-1 Class II, division 1 malocclusion in the deciduous dentition (compare with Fig 2-26). (a and b) The position of the mandibular dental arch is too far posterior in relation to the maxillary dental arch. The deciduous molars are in adequate transverse occlusion. The mandibular dental arch has a normal width; the maxillary dental arch is slightly too narrow. (b) The overjet is too large. (c) The overbite is small. (d) The mandibular posterior teeth occlude too far to the distal. The terminal plane of the deciduous dentition has a distal step.
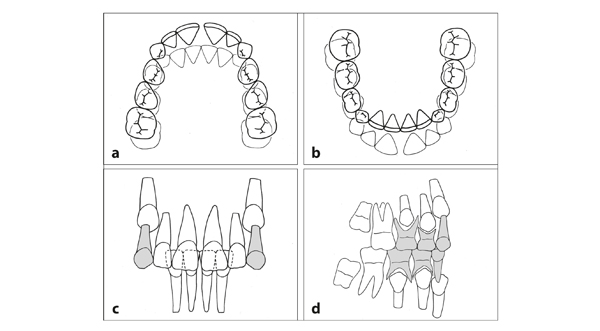
Fig 11-2 Class II, division 1 malocclusion in the intertransitional period (compare with Fig 4-1). (a and b) The distoclusion coincides with an abnormally large overjet, a small and tapering maxillary dental arch, and an adequate transverse occlusion. (c) The permanent incisors erupt until they are vertically supported. There is a large overbite. The ed/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


