5 Orofacial Complex: Form and Function
This chapter discusses primarily the physiological form of the teeth and periodontium, with consideration of the coverage of form and function in Chapter 4 and the coverage of orofacial structures in other chapters on muscles and joints.
Form and Function
The phrase form and function reflects a concept of interrelation of the shape or attributes of something with its function. In dentistry the phrase may indicate the entire masticatory system, acting as a biomechanical engine for the reduction of food. If so, then arguably it may be possible to try to make a case that each of the components of the masticatory system has some kind of physiological relationship to its individual functions and to that of the whole system, including its maintenance. These relationships have a spectrum of possible associations: speech and jaw motion1; arch form and mathematical function2; integration of form, function, and esthetics in mandibular anterior ceramic veneers3; morphological and functional analysis of the orofacial complex4; and the condylar disk as the controlling factor in the form of the condylar head.5 The search for the meaning of form and function continues.
Form Follows Function
For some clinicians the general principle that becomes operant is form follows function, which means, for example, that in restorative dentistry, the dependent relationship between the original biomechanical behavior of stress concentrations in incisor teeth6 and the nature of the materials used to restore these teeth is addressed. Thus the term form not only means shape but also biomechanical attributes that contribute to the maintenance of function. Other examples include the dependent relationship between esthetics and optimum occlusion,7 physical forces and the periodontal ligament,8 and arch form and beta function,2 as well as the controversial interrelationship between the morphology and function of the discomuscular apparatus of the human temporomandibular joint. Although the function of implant-supported restorations seems to be generally achieved, the esthetics and biocompatibility of the materials used (i.e., design and fabrication of restorative components with dimensions that closely resemble natural tooth anatomy and esthetics) remain a challenge.9,10
Articulation of Teeth
Anyone who has carved a set of Ivorine teeth, even to the dimensions set forth in Table 1-1, can attest to the difficulty of aligning the carved teeth into what might be thought to be only one proper articulation of the teeth on an articulator. Form and function are not a template by which it is possible to draw a straight-line correlation between the shape of a tooth and all of its functions. A restored crown of a maxillary central incisor should meet standards of function and esthetics (see Figure 1-1).
Fundamental Curvatures
Although a great deal has been said about the relationship of the health of the gingiva to the contours of the teeth, as indicated in the references included at the end of this chapter, such appraisals are generally descriptive, involve restorations, and are retrospective observations. To conclude that the gingival tissues around a tooth (natural or restored) need neither stimulation nor protection suggests that the true significance of buccolingual crown contours has not been evaluated. In no instance has the influence of axial contours, which begin with the height of the contour of buccal and lingual surfaces, been tested in relation to such functions as chewing efficiency or occlusal stability. And even though the significance of buccolingual crown contours to gingival health relative to gingival stimulation, self-cleansing mechanisms, and gingival protection has been seriously questioned, the significance of other contours has also been questioned. Dental plaque accumulates on teeth in the absence of adequate oral hygiene, and gingivitis occurs in spite of “self-cleansing” mechanisms.11 The influence of a primitive diet does not appear to prevent gingivitis. However, plaque formation and gingivitis may be related more to bacterial attachment mechanisms, bacterial toxins, and food substrates than to physical form. It should not be concluded from such observations that curvatures have nothing to do with the function and health of the masticatory system. The effect of overcontouring or undercontouring of surfaces of the teeth may be related more to occlusal mechanisms than to self-cleansing mechanisms and be of more significance to food self-cleansing efficiency and/or musculature in one patient than in another. The role of protective reflexes in relation to the contours of the teeth is not known. Even though the significance of tooth forms has yet to be clarified, ideas about form and function that have been held should be understood, and liberties with form avoided. The following are considered:
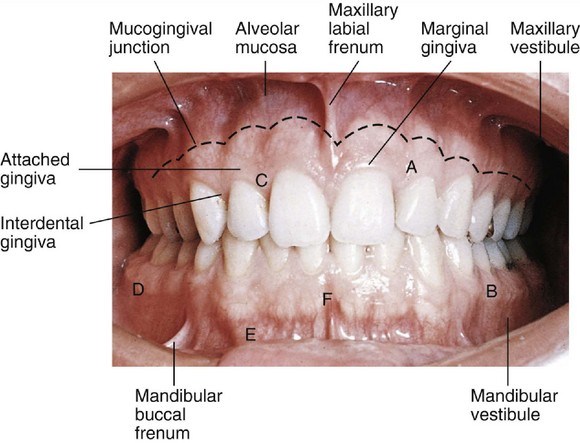
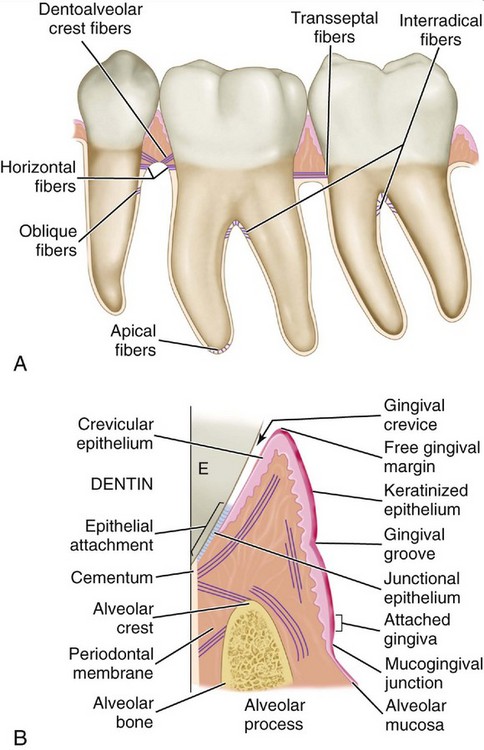
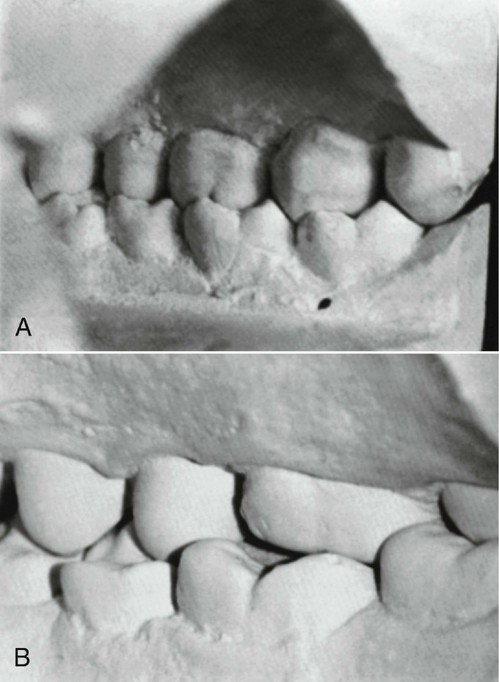
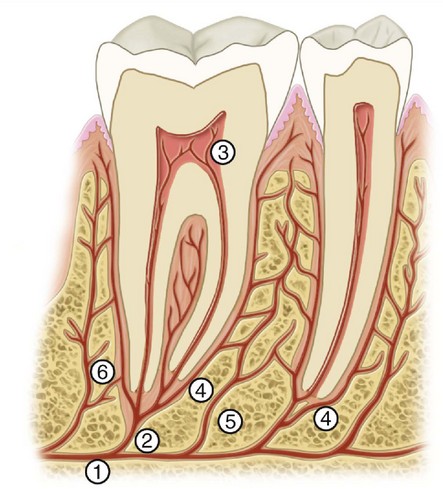
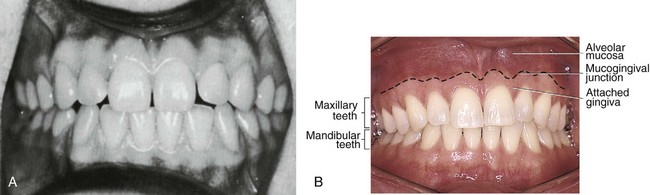
These headings include form, which has been considered to have a direct or primary bearing on the protection of the periodontium. Many other details of tooth form may have an indirect bearing on the stability of the teeth through their contribution to the maintenance of efficiency during function. Some of these details are cusp forms, the proportions of various measurements of the crowns and roots, root form, and anchorage and angles at which teeth are set in the jaws. It has been suggested that when well-formed teeth are in normal alignment with normal gingival contour (Figures 5-1 and 5-2), the efficient use of the toothbrush during home care of the teeth is enhanced.11
Proximal Contact Areas
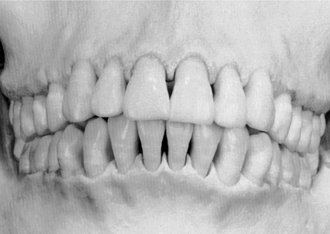
Soon after the alignment of all of the teeth in their respective positions in the jaws takes place, a positive contact relation of one tooth with another in each arch should be established mesially and distally (Figure 5-3). Except for the last molars (third molars, if present), each tooth has two contacting members adjoining it. The last molar is in contact only with the tooth mesial to it. Although the areas of contact are still very circumscribed, especially on anterior teeth, these are areas and not mere points of contact (Figure 5-4). Actually, the term contact point, which is often used to designate the contact of teeth in the same arch, is a misnomer. When the individual is quite young and the teeth are newly erupted, some of the teeth come close to having point contacts only when the contacting surfaces are nearly perfect curvatures. Examples of the few contacts made by such rounded surfaces are contacts located distally on canines and mesially on first premolars, maxillary and mandibular.
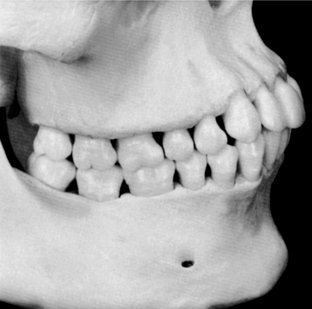

The proper contact relation between neighboring teeth in each arch is important for the following reasons: it serves to keep food from packing between the teeth, and it helps stabilize the dental arches by the combined anchorage of all the teeth in either arch in positive contact with each other (Figures 5-5 and 5-6; see also Figure 5-3). Except for the third molars, each tooth in the arch is supported in part by its contact with two neighboring teeth, one mesial and one distal. The third molars (and the second molars if no third molar is present) are prevented from drifting distally where there is no contacting tooth by the angulation of their occlusal surfaces with their roots and by the angle of the direction of the occlusal forces in their favor. This is explained more fully in later chapters.
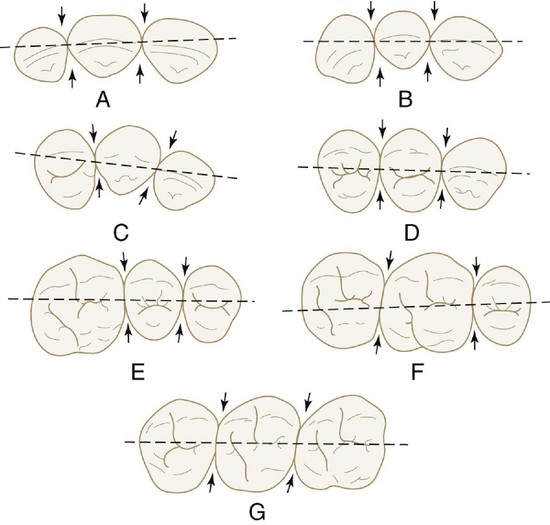
Contact areas must be observed from two aspects to obtain the proper perspective for locating them: the labial or buccal aspect, and the incisal or occlusal aspect (Figures 5-7 and 5-8).
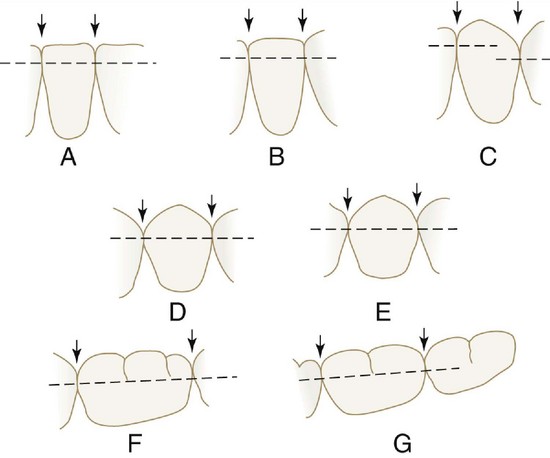
The labial or buccal view will demonstrate the relative positions of the contact areas cervicoincisally or cervico-occlusally. The center of the area from this aspect is gauged by its relation to the length of the crown portion of the tooth (Figure 5-9).
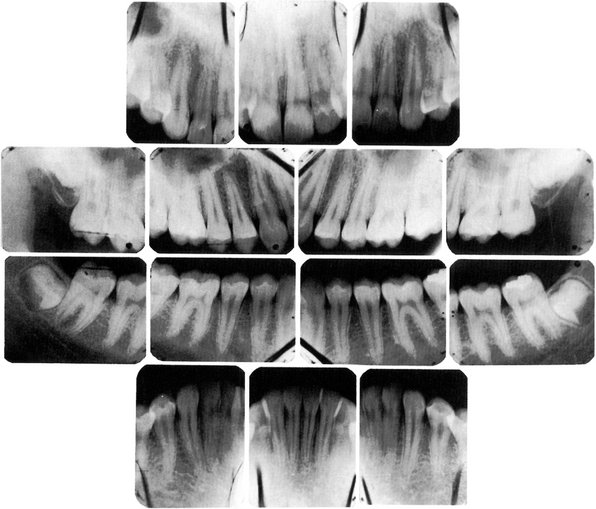
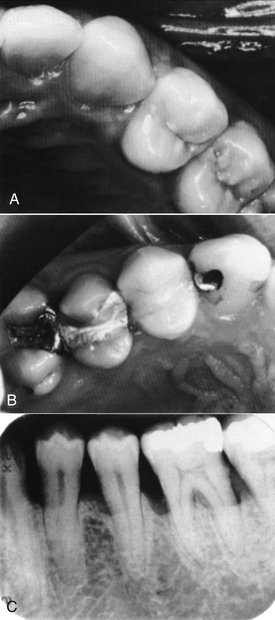
Figure 5-9 Radiograph demonstrating form of alveolar crest, contact areas, and relation to form of the crown.
The incisal or occlusal view will show the relative position of the contact areas labiolingually or buccolingually. In this instance, the center of the area may be located in its relation to the labiolingual or buccolingual measurement of the crown (Figure 5-10; see also Figure 5-8). The point at which the contact area is bisected also depends on the outline of the form of the crown from the incisal or occlusal aspect. This outline is governed by the alignment of the tooth in the arch and also by the occlusal relation with its antagonists in the opposing arch. The mandibular first molar is an excellent example (Figure 5-11; see also Figure 5-10). The contact and embrasure design for this tooth is explained later when the incisal and occlusal aspects of the teeth are considered.


Interproximal Spaces (Formed by Proximal Surfaces in Contact)
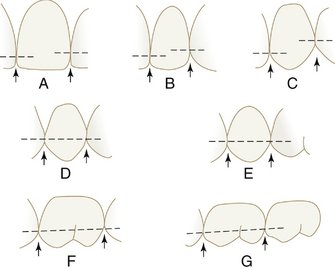
The interproximal spaces between the teeth are triangularly shaped spaces normally filled by gingival tissue (gingival papillae). The base of the triangle is the alveolar process, the sides of the triangle are the proximal surfaces of the contacting teeth, and the apex of the triangle is in the area of contact. The form of the interproximal space will vary with the form of the teeth in contact and will depend also on the relative position of the contact areas (Figures 5-12 through 5-14). Normally, a separation of 1 to 1.5 mm exists between the enamel and alveolar bone. Thus the distance from the CEJ (cervical line) to the crest of the alveolar bone as seen radiographically (see Figure 5-9) is 1 to 1.5 mm in a normal occlusion in the absence of disease.
Because the teeth are narrower at the cervix mesiodistally than they are toward the occlusal surfaces and the outline of the root continues to taper from that point to the apices of the roots, considerable spacing is created between the roots of one tooth and the roots of adjoining teeth. This arrangement allows sufficient bone tissue between one tooth and another, which anchors the teeth securely in the jaws. It also simplifies the problem of space for the blood and nerve supply to the surrounding alveolar process and other investing tissues of the teeth (see Figure 5-12).
Embrasures (Spillways)
When two teeth in the same arch are in contact, their curvatures adjacent to the contact areas form spillway spaces called embrasures. The spaces that widen out from the area of contact labially or buccally and lingually are called labial or buccal and lingual interproximal embrasures. These embrasures are continuous with the interproximal spaces between the teeth (see Figure 5-10). Above the contact areas incisally and occlusally, the spaces, which are bounded by the marginal ridges as they join the cusps and incisal ridges, are called the incisal or occlusal embrasures. These embrasures, and the labial or buccal and lingual embrasures, are continuous (Figure 5-15; see also Figure 5-8). The curved proximal surfaces of the contacting teeth roll away from the contact area at all points, occlusally, labially or buccally, and lingually and cervically, and the embrasures and interproximal spaces are continuous, as they surround the areas of contact.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


