16 Occlusion
The definition of the term occlusion in many dictionaries only states that it is the act of closure or being closed, but some dental dictionaries (e.g., Zwemer1) go well beyond this simple definition to include a static, morphological tooth contact relationship. It may be defined also as the contact relationship of the teeth in function or parafunction.2 However, the term refers not only to contact at an occlusal interface, but also to all those factors concerned with the development and stability of the masticatory system and with the use of the teeth in oral motor behavior. Because brief definitions of occlusion are too limited to be useful as a basis for dental practice, more complete explanations evolve into concepts or paradigms of occlusion that reflect prevailing interests and clinical convenience. Thus a modern concept of occlusion must include the idea of an integrated system of functional units involving teeth, joints, and muscles of the head and neck. The solutions to problems such as bruxism, orthodontic relapse, denture instability, and periodontal trauma require concepts of occlusion that extend well beyond static arrangements of teeth, occlusal contacts, and jaw position.
Concepts of Occlusion
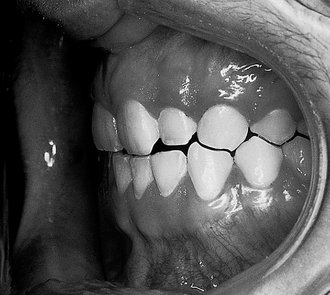
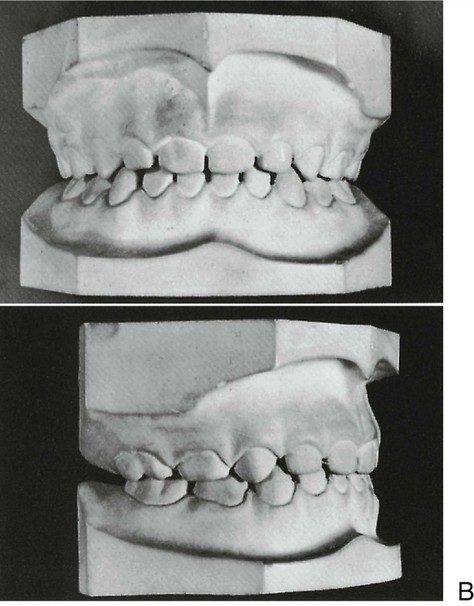
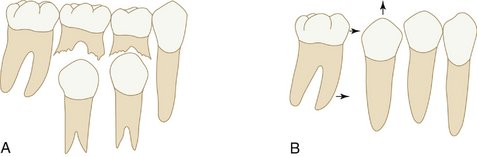
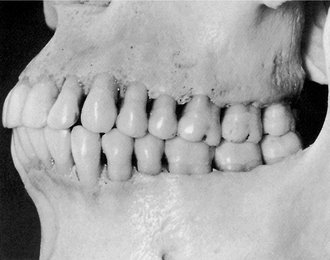
In the past, ideas regarding occlusion were often based on complete dentures. Because of the problems of instability of denture bases, the concept of “balanced occlusion” was developed to consider bilateral contacts in all functional excursions to prevent tipping of the denture bases. Although some clinicians have advocated such concepts in the past for use with regard to the natural dentition, acceptance was limited and unsupported by research evidence. Even so, some of the concepts related to condylar guidance, cusp height, incisal guidance, curve of Spee, and plane of occlusion have been useful in the restoration of natural teeth. Several concepts of an “ideal” or optimal occlusion of the natural dentition have been suggested by Angle,3 Schuyler,4 Beyron,5 D’Amico,6 Friel,7 Hellman,8 Lucia,9 Stallard and Stuart,10 and Ramfjord and Ash.11 These concepts stress to varying degrees static and/or functional characteristics of an occlusion as being theoretical practical goals for diagnosis and treatment of the occlusion. Some of the ideas have been developed principally in relation to orthodontics or complete dentures, and others for full mouth rehabilitation. None are completely applicable to the natural dentition; some provide for specific occlusal contact relations and joint positions, and few concepts of occlusion consider in principle, or in practical ways, related muscle and oromotor functions. The idea of a functional rather than simply a static relationship of occlusal surfaces has become increasingly important because of the recognition that functional disturbances of the masticatory system can be related to malocclusion, occlusal dysfunction, and disturbances of oral motor behavior, including bruxism. Thus, for example, the occlusal contact relationships shown in Figure 16-1 reflect oromotor behavior consistent with bruxism (grinding of the teeth) that requires preventive occlusal therapy to control its adverse effects (e.g., an occlusal bite plane stabilization–type splint) (Figure 16-2). The restoration of lost tooth structure due to aggressive bruxism, as for other losses from other causes, requires knowledge of dental morphology, physiology, restorative materials, occlusion, esthetics, and personal habits (e.g., pipe smoking).

Primary Dentition
OVERVIEW OF THE PRIMARY OCCLUSION
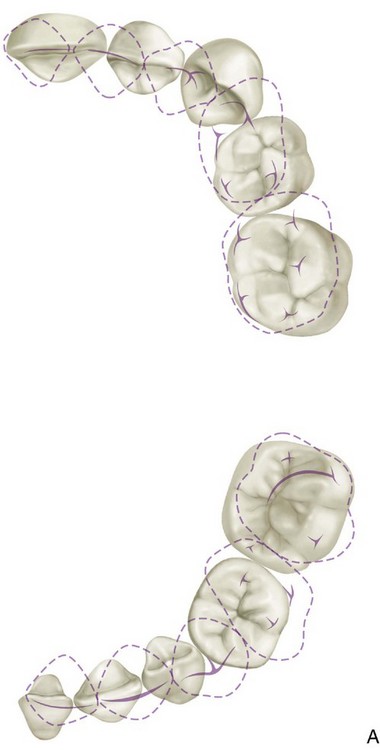
The primary teeth are arranged in the jaws in the form of two arches: a maxillary and a mandibular. An outline following the labial and buccal surfaces of the maxillary teeth describes the segment of an ellipse and is larger than the segment following the same surfaces on the mandibular teeth (see Figure 1-2, A).
ERUPTION CHRONOLOGY OF THE PRIMARY TEETH
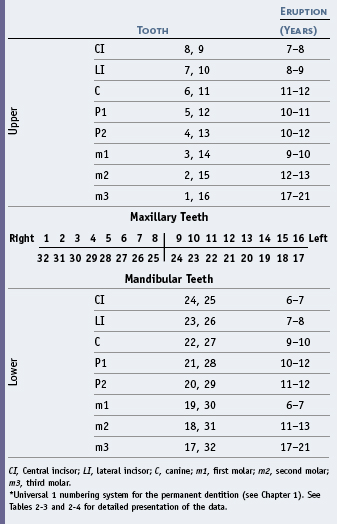
The chronology of the emergence/eruption of the primary teeth, which is shown in Table 16-1, is derived from data provided in Chapter 2.

The timing of the eruption or emergence of the teeth is due in large part to heredity and only somewhat to environmental factors. According to Falkner12 the development and eruption of the primary dentition are quite independent of the development and maturation of the child as a whole. The significance of local environmental factors for the development of occlusion considered in its broadest sense is relatively unknown. Thus learning of mastication may be highly dependent on the stage of development of the occlusion (type and number of teeth present), maturation of the neuromuscular system, and factors such as diet.
MEAN AGE OF ERUPTION
The mean age of eruption of the primary teeth as shown in Table 16-1 is demonstrated schematically in Figure 16-3, although one should keep in mind the range of values seen in Table 16-1 and the idea that a 6-month acceleration or delay is considered normal. Even so, on average the sequence generally follows that shown in Figure 16-3.
PRIMARY ARCH FORM
The arch form and width for both the primary and permanent dentitions has been largely established by the age of 9 months.13 This observation may seem untrue in view of the apparent difference in facial appearance between the child of that age and a young adult with a permanent dentition. What does change substantially, of course, is the anteroposterior dimension of the jaws, an increase in which is necessary for the incorporation of the permanent molars into the occlusion. It must be kept in mind that the alveolar bone and basal bone determine the shape of the dental arches. Arch form will be considered in more detail in the section on the permanent dentition.
INTERDENTAL SPACING
The position of the deciduous teeth in the arches generally shows some degree of interdental spacing, which tends to decrease slightly with age. The size of the primary teeth and the spacing between them has a relationship to the position of the permanent teeth and the size of the dental arches (e.g., sufficient interdental space is needed for the permanent teeth to erupt into an uncrowded position). One of the indicators of future sufficiency or insufficiency of space in the dental arches for the permanent teeth is the presence or absence of spacing between the teeth of the primary dentition14,15 (i.e., spacing between the primary teeth [Figure 16-4] is necessary for the proper alignment of the permanent dentition).

The probability of crowding of the permanent dentition based on the amount of interdental spacing of the primary teeth is given in Table 16-2.
Table 16-2 Probability of Crowding of Permanent Teeth Based on Available Spaces Between Primary Teeth
| Primary Teeth | Chances of Crowding |
|---|---|
| >6 mm | None |
| 3–5 mm | 1 in 5 |
| >3 mm | 1 in 2 |
| No spacing | 2 in 3 |
| Crowded | 1 in 1 |
Data from Leighton BC: The early signs of malocclusion, Trans Eur Orthod Soc 45:353, 1969; and Leighton BC: Early recognition of normal occlusion. In McNamara JA Jr, editor: Craniofacial growth series: the biology of occlusal development, Monograph 7, Ann Arbor, 1977, Center for Human Growth and Development, University of Michigan.
PRIMARY MOLAR RELATIONSHIPS
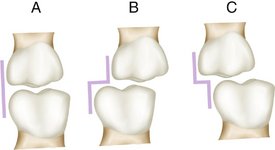
Primary molar relationships have been described by Moyers as the flush terminal plane, mesial step, and distal step (Figure 16-5, A, B, and C).14 Of particular interest to the orthodontist is the fact that the mandibular second primary molar has a greater mesiodistal diameter than the maxillary second molar. As a result of this difference in dimensions of the two teeth, the distal surfaces of these two molars are in the same plane; a flush terminal plane is located at the end of the deciduous dentition. It has been reported that if a “step” (deviation of the flush terminal plane) occurs because of carious lesions or other disturbances, a tendency to interfere with the development of normal occlusal relations of the permanent first molars is evident. Also, it has been shown that the natural wearing away of the cusps in the deciduous dentition allows the mandible to assume a more forward position during a period when the mandible is growing more rapidly than the maxilla. In the absence of cuspal interferences, there is some evidence that the permanent incisors erupt with less vertical overlap and the permanent molars erupt into a more favorable occlusion. Several orthodontic techniques have been directed toward the functional protraction of the mandible during growth in patients with anteroposterior jaw discrepancies.
EFFECTS OF TERMINAL PLANE RELATIONSHIPS
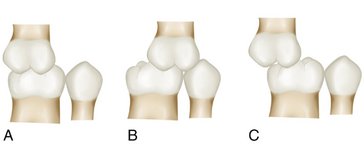
The effect of these deciduous molar relationships (see Figure 16-5) on the development of relationships of the permanent molars (Figure 16-6) is influenced to some degree by the presence or absence of several factors: differential growth of the jaws, forward growth of the mandible, and sufficient leeway space to accommodate a mesial shift of the permanent molars.16 Morphological growth studies on the growth process of a primary dentition having a distal step have been reported by Inuzuka17 and Bishara et al.18 In the latter study it was found that more than 60% of the subjects in the study developed a Class I molar relationship (see Figure 16-6, A; see also Figure 16-31), almost 35% developed a Class II relationship (see Figure 16-6, B), and slightly more than 4% developed a Class III molar relationship (see Figure 16-6, C). The sides of the arch that started with a distal step in the deciduous dentition proceeded to develop into a Class II molar relationship in the permanent dentition. Of the sides with a flush terminal plane, 56% progressed into a Class I molar relationship and 44% into a Class II molar relationship. The mesial step in the deciduous dentition indicates a greater probability for a Class I molar relationship and a lesser probability for a Class III molar relationship. The Class I molar relationship is considered to be a “normal” relationship (i.e., the mesial buccal cusp of the maxillary molar occludes in the mesiobuccal developmental groove of the first permanent molar) (see Figure 16-6, A). The completion of the eruption of the primary teeth into occlusion results in the contact relations shown in the section on the permanent dentition.
DETAILS OF THE PRIMARY OCCLUSION
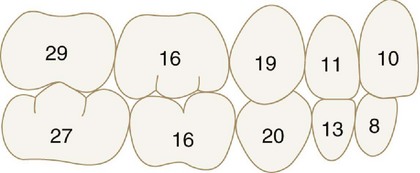
The occlusion of the primary teeth in a 3-year-old child is described. After separation has begun, the migration of the teeth changes the occlusion. Nevertheless, if development is normal, the spacing of the teeth is rather uniform (Figure 16-7). This biological change opens up contacts in the arch between teeth and increases occlusal wear. These changes anticipate the child’s needs, however, because if normal healthy reactions are in effect, the child seldom suffers from mechanical irritations during this severe adjustment period.

Figure 16-7 Primary/deciduous dentition.
(From Ash MM, Ramfjord S: Occlusion, ed 4, Philadelphia, 1995, Saunders.)
The normal occlusion of the primary teeth at the age of 3 years is as follows.
The interrelation of cusps and incisal ridges of the opposing arches of primary teeth may be studied in Figure 16-8. The size relation of deciduous and permanent arches is illustrated in Figure 16-9 (see also Figure 1-2).
Mixed (Transitional) Dentition
The transition from primary to permanent dentition begins at about 6 years of age with the emergence of the mandibular permanent central incisors (Figures 16-10 and 16-11) or the first permanent molars at 6 to 7 years of age. The timing of the shedding of the primary teeth has an effect on the emergence of the permanent teeth (i.e., early shedding of primary teeth advances the emergence of the permanent teeth).19

Figure 16-10 Observe available space and size of emerging permanent incisors and incisal edge mamelons. Child is 6.5 years of age.
(From Ash MM, Ramfjord S: Occlusion, ed 4, Philadelphia, 1995, Saunders.)
ARCH DIMENSIONS AND TOOTH SIZE
The growth of the jaw provides space for the teeth to erupt and emerge into the mouth. Forward rotation of the maxillomandibular complex, which is the more usual pattern, influences the magnitude of tooth eruption as well as the ultimate anteroposterior position of the incisors. Lingual positioning of the mandibular incisors relative to the mandible often accompanies forward rotation during growth.20,21 Changes in the anteroposterior position of the incisors with rotation reflect a major influence on changes in arch length. It has been suggested that changes in arch length, which occur in both arches with rotation during growth associated with movement of the incisors, may be of relatively greater importance than forward movement of the molars.15
An important portion of the dental arch in the development of the occlusion of the permanent dentition is the premolar segment. In this section, the erupting premolars are significantly smaller in mesiodistal dimension than the primary molars, which they replace. The dynamics of this change in arch dimensions, particularly in the mandibular arch, is important to a proper understanding of the development of occlusion and malocclusion. An often-confusing point in the analysis of the mixed dentition is the actual decrease in arch perimeter during the growth of the mandible. The arch perimeter of the permanent dentition, as measured from the mesials of the mandibular first molars, decreases an average of about 4 mm.22 This occurs at the same time that the mandible and basal bone are experiencing significant growth posteriorly. Because this change is found to a greater extent in the mandible than in the maxilla and because of the pronounced tendency for the lower molars to drift mesially, occlusal relationships are in a flux during the later stages of the mixed dentition.
When a discrepancy is evident between the aggregate mesiodistal dimension of the teeth and the size of the bony supporting arches, crowding or protrusion can occur. The discrepancy may relate to small or large teeth, small or large bony bases, or some combination of these dimensions. It was shown by Howe et al23 that arch width and perimeter dimensions can relate to differences between crowded and uncrowded dentitions.
ARCH WIDTH
Arch width is measured between corresponding lingual points (e.g., intersection of the lingual groove and gingival margin) on the teeth in the same arch (e.g., transpalatal width between second molars). Maxillary intermolar width, for example, can be as much as 6 mm less in crowded dentitions than in uncrowded dentitions. A transpalatal width increase of 2.5 to 3.0 mm occurs in untreated persons from 7 to 15 years of age. According to a study by Spillane and McNamara,24 if an inadequate transpalatal width is evident in a narrow dental arch (less than 31 mm) in the early mixed dentition, it is unlikely that the child will reach adequate arch dimensions through normal growth mechanisms. The distance (perimeter) around the dental arch as measured from the mesial surfaces of right and left maxillary second molars is significantly greater in uncrowded dentitions than in crowded dentitions. Other researchers have obtained similar findings. Orthodontists undertake the prevention or treatment of tooth and arch size discrepancies. However, it is in the best interests of their patients for practitioners to know something of the significance of the differences in size between the primary/deciduous teeth and the permanent teeth and between tooth size and arch size.
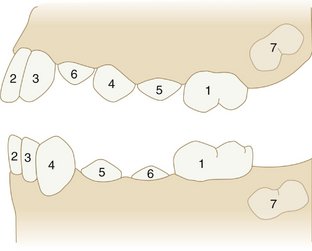
DIFFERENCES IN TOOTH SIZE
The relationship of the size of the dental arches to differences between the size of the primary/deciduous teeth and the size of the permanent teeth is important relative to the development of the permanent dentition. For example, the aggregate size of the posterior permanent teeth is generally smaller in the mesiodistal dimension than that of the primary teeth, and the posterior succedaneous teeth (permanent teeth) generally have a smaller total mesiodistal dimension than the primary teeth. The difference is related to the leeway space, or the amount of space gained by the difference in the mesiodistal dimensions of the premolars and the primary molars.14,15 The average mesiodistal size of the primary dentition in that area is 47 mm, which, when compared with the succeeding aggregate tooth dimension of 42.2 mm, indicates an average gain of 4.8 mm in available space. In effect, the difference in size of the posterior succedaneous/permanent teeth and the primary teeth provides for the mesial movement of the permanent molars (Figure 16-12). Thus a simple comparison of tooth size of the two dentitions can indicate a need for additional space in both dental arches as soon as the primary incisors are lost, except when sufficient interdental spacing is evident in the primary dentition.25
Some of the space made available by the leeway space (the difference in sizes between the premolars and primary molars) must be used for alignment of the lower incisors, because these teeth erupt with an average of 1.6 mm of crowding.26 The mandibular molar will use the remainder of the space. This movement of the mandibular molar may correct an end-to-end molar relationship (normal for the mixed dentition) into a normal molar relationship in the permanent dentition (i.e., the mesial lingual cusp of the maxillary first molar occludes in the central fossa of the mandibular first molar and the mesial buccal cusp of the maxillary first molar occludes between the mesial and distal buccal cusps of the mandibular first molar) (see Figure 16-27).
INCISAL LIABILITY
If the second molars erupt before the premolars erupt fully, a significant shortening of the arch perimeter occurs, and malocclusion may be more likely to occur.27 Because of the discrepancy in mesiodistal crown dimensions between the primary and permanent incisors, some degree of transient crowding may occur (incisal liability) at about the age of 8 to 9 and persist until the emergence of the canines, when the space for the teeth may again be adequate.
Permanent Dentition
The sequence of eruption of the permanent dentition is more variable than that of the primary dentition and does not follow the same anteroposterior pattern. In addition, significant differences in the eruption sequences between the maxillary arch and the mandibular arch do not appear in the eruption of the primary dentition (Table 16-3).
The most common sequences of eruption in the maxilla are 6-1-2-4-3-5-7-8 and 6-1-2-4-5-3-7-8. The most common sequences for the mandibular arch are (6-1)-2-3-4-5-7-8 and (6-1)-2-4-3-5-7-8.28 These are also the most favorable sequences for the prevention of malocclusion (Figure 16-13). As noted earlier, should the second molars erupt before the premolars are fully erupted, significant shortening of the arch perimeter resulting in malocclusion is likely to occur, even if the alveolar bone arch dimensions are adequate for the size of the permanent dentition.27
DENTAL ARCH FORM
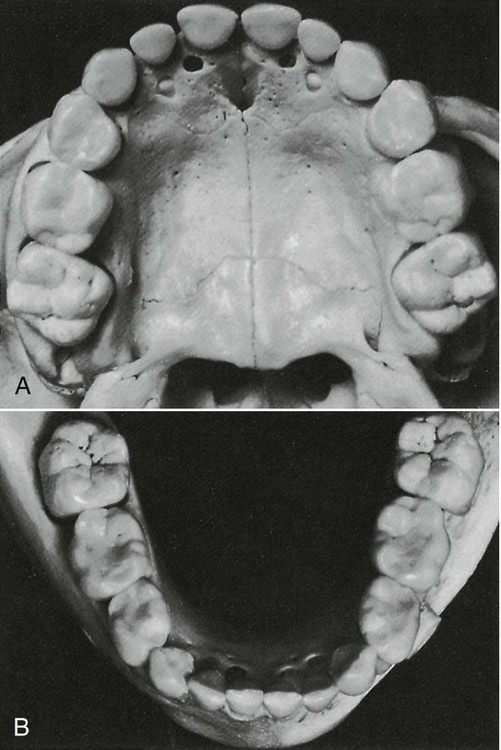
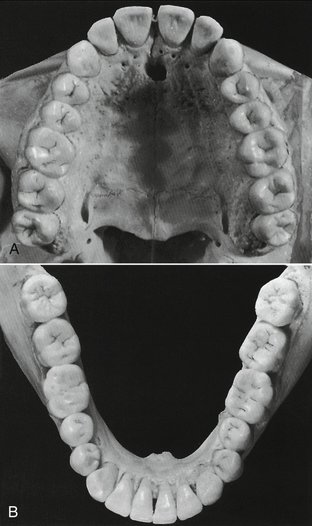
The teeth are positioned on the maxilla and mandible in such a way as to produce a curved arch when viewed from the occlusal surface (Figure 16-14). This arch form is in large part determined by the shape of the underlying basal bone.
Malpositioning of individual teeth does not alter the arch form. When multiple teeth are misplaced, however, then irregularities or asymmetries may develop in arch form. A tapered arch form generally occurs in the maxillary arch and is quite often the result of a pathological narrowing of the anterior maxilla. Less commonly, a severe thumb-sucking habit may result in arch narrowing of the anterior maxilla (Figure 16-15).

Figure 16-15 Anterior open bite.
(From Dawson PE: Functional occlusion: from TMJ to smile design, ed 1, St Louis, 2007, Mosby.)
The basic pattern of tooth position is the arch. On the basis of qualitative observations, anthropologists have described the general shape of the palatal arch as being paraboloid, U-shaped, ellipsoid, rotund, and horseshoe-shaped.29,30 An arch has long been known architecturally (as the word architecture itself implies) as a strong, stable arrangement with forces being transmitted normal to the apex of a catenary curve.31,32 The shape of the arch form of the facial surfaces of the teeth was thought by Currier33 to be a segment of an ellipse. In the past, interest in arch form was directed toward finding an “ideal” or basic mean arch form pattern that functionally interrelates alveolar bone and teeth and could have clinical application. However, any ideal arch pattern tends to ignore variance, a clinical reality which suggests that adaptation mechanisms are more important for occlusal stability than any ideal template.
OVERLAP OF THE TEETH
The arch form of the maxilla tends to be larger than that of the mandible. As a result, the maxillary teeth “overhang” the mandibular teeth when the teeth are in centric occlusion (the position of maximal intercuspation). The lateral or anteroposterior aspect of this overhang is called overjet, a term that can be made more specific as indicated in Figure 16-16. This relationship of the arches and teeth has functional significance, including the possibility of increased duration of occlusal contacts in protrusive and lateral movements in incising and mastication.
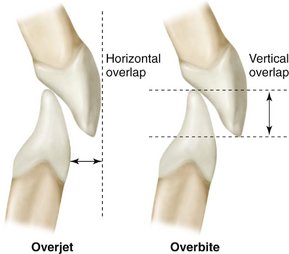
Figure 16-16 The terms overjet and overbite are commonly used to describe horizontal and vertical overlap of teeth.
The significance of vertical and horizontal overlap has to be related to mastication, jaw movements, speech, type of diet, and esthetics. Excessive vertical overlap of the anterior teeth may result in tissue impingement and is referred to as an impinging overbite (Figure 16-17). Correction is not simply a matter of trying to increase vertical dimension by restorations on posterior teeth. Orthodontics is generally required, and sometimes orthognathic surgery is recommended.

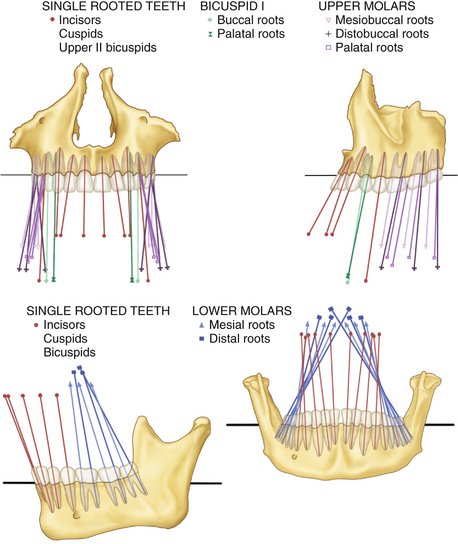
CURVATURES OF OCCLUSAL PLANES
The occlusal surfaces of the dental arches do not generally conform to a flat plane (e.g., the mandibular arch has one or more curved planes conforming to the arrangement of the teeth in the dental arches). Perhaps the most well known is the curve of von Spee, who noted that the cusps and incisal ridges of the teeth tended to display a curved alignment when the arches were observed from a point opposite the first molars. This alignment (Figure 16-18) is spoken of as the compensating curve or curve of Spee.34 This curvature is within the sagittal plane only. Monson35 visualized a three-dimensional spherical curvature involving both the right and left bicuspid and molar cusps and the right and left condyles. It was supposed that the center of a sphere with an 8-inch diameter was the vector for converging lines of masticatory forces passing through the center of the teeth and that the occlusal surfaces of the molar teeth were congruent with the surface of a sphere of some dimension. This hypothesis was not supported by research by Dempster et al36 (i.e., the longitudinal axes of the roots of the teeth do not converge toward a common center) (Figure 16-19). Although the idea was incorporated into complete dentures and the design of some early articulators,37,38 such curvature has not been accepted as a goal of treatment even for dentures. However, the curvature of the occlusal plane such as the curve of Spee does have clinical significance in relation to tooth guidance—that is, canine and/or incisal guidance as applied in orthodontics and restorative dentistry. In these, disocclusion of the posterior teeth is desired during anterior (protrusive) movements.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


