Orthodontic treatment in patients with congenitally missing teeth can be challenging. In this case report, we describe the treatment of a 15-year-old girl with mild dental crowding and 2 congenitally missing mandibular incisors. The Forsus fatigue-resistant device was used to move the mandible and the mandibular teeth forward. A new balanced and stable occlusion was achieved after treatment. When the treatment plan includes moving the mandibular teeth forward in a patient with mandibular incisor agenesis, the profile and the skeletal and dental features should be carefully scrutinized to ensure that balanced and esthetic results are achieved.
Hypodontia is the congenital absence of at least 1 tooth. Orthodontic treatment in patients with congenitally missing teeth can be challenging. The prevalence of hypodontia varies among different ethnicities. The most commonly missing teeth for white populations are the maxillary lateral incisors and the second premolars (third molars excluded). However, in Chinese, Korean, and Japanese populations, agenesis of the mandibular incisors is more frequently observed. Mandibular incisor agenesis might be caused by heredity, anomalies of the mandibular symphysis, dentition reduction of an evolutionary trend, or localized inflammation. Patients with congenitally missing mandibular incisors usually show retroclination of the mandibular incisors and reduction of the mandibular alveolar bone area.
Three treatment modalities are common for patients with agenesis of the mandibular incisors. One involves creating space for a fixed denture or an implant restoration, which could help achieve a satisfactory occlusion. Another choice is extraction of the maxillary incisors or premolars to reduce the severe deep overjet by retracting the anterior teeth. The third option is to create a new balanced occlusion by closing the spaces and moving the mandibular canines and the posterior teeth forward.
The Forsus fatigue-resistant device (FRD; 3M Unitek, Monrovia, Calif) is a semirigid fixed functional appliance. It is used most frequently for treating Class II patients. As claimed by the manufacturer, the Forsus FRD can exert consistent forces and is resistant to fracture. It consists of superelastic nickel-titanium coil springs that can be assembled at chairside. Recent studies have reported that the Forsus FRD can restrain sagittal growth of the maxilla, stimulate mandibular growth, and induce mesial movement of the mandibular teeth and distal movement of the maxillary molars.
We present the treatment of a patient with a Class I malocclusion with 2 congenitally missing mandibular incisors. The treatment plan involved forward movement of the mandible and the mandibular teeth to reduce the deep overjet using the Forsus FRD appliance.
Diagnosis and etiology
The patient was a 15-year-old girl with a chief complaint of dental crowding. She was in good health with no significant systemic medical history. No oral habits and no temporomandibular joint (TMJ) symptoms were noted.
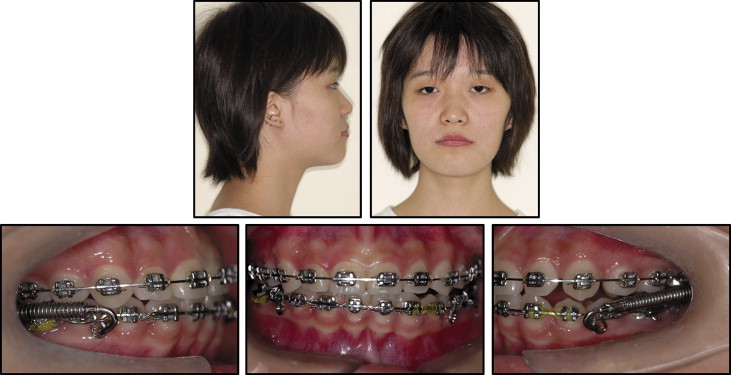
The pretreatment facial frontal photographs showed a well-balanced and symmetric face ( Fig 1 ). Her profile was straight with competent lips, a good chin-throat soft-tissue line, a proper nasolabial angle, and normal vertical proportions. The molar relationships were Class I on both sides. The anterior overbite was deep, with the maxillary incisors overlapping the mandibular incisors by 50%. Anterior overjet was 3 mm. Her maxillary midline was coincident with the facial midline, and the mandibular midline was shifted 1 mm to the left. Both arch forms were U-shaped. There was 5.5 mm of crowding in the maxillary arch. The mandibular central incisors were congenitally missing ( Fig 2 ).

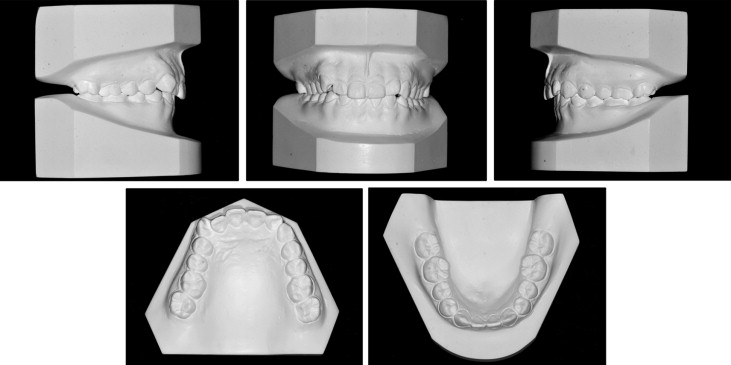
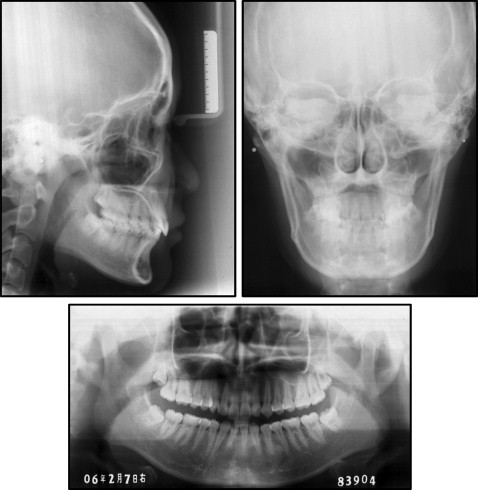
The panoramic radiograph confirmed the absence of the 2 mandibular incisors. Four third molars were present, with the mandibular right third molar inclined forward ( Fig 3 ). The cephalometric analysis showed a Class II skeletal base with a low mandibular plane angle. The maxillary incisors were tipped lingually, and the mandibular incisors were labially proclined ( Table ). No obvious asymmetries were seen in the anteroposterior radiograph ( Fig 3 ).
| Norm | Pretreatment | Posttreatment | Follow-up at 6 months | Follow-up at 42 months | |
|---|---|---|---|---|---|
| SNA (°) | 82.8 ± 4.0 | 84.1 | 85.6 | 84.1 | 84.5 |
| SNB (°) | 80.1 ± 3.9 | 78.6 | 80.7 | 79.5 | 79.3 |
| ANB (°) | 2.7 ± 2.0 | 5.5 | 4.9 | 4.6 | 5.2 |
| Wits (mm) | −1.1 ± 2.9 | 3.6 | 1 | 2.8 | 2.6 |
| MP-SN (°) | 32.5 ± 5.2 | 27.6 | 27.5 | 27.8 | 28.2 |
| PP-MP (°) | 27.6 ± 4.6 | 17.5 | 16.5 | 17.5 | 17.5 |
| L1-NB (mm) | 6.7 ± 2.1 | 5.0 | 8.5 | 8.2 | 7.5 |
| L1-NB (°) | 30.3 ± 5.8 | 28.4 | 34.2 | 34.5 | 35.7 |
| IMPA (°) | 93.9 ± 6.2 | 102.5 | 106.4 | 107.5 | 110.5 |
| U1-NA (mm) | 5.1 ± 2.4 | 2.5 | 5.0 | 5.0 | 4.5 |
| U1-NA (°) | 22.8 ± 5.7 | 20.7 | 30.3 | 31.0 | 29.2 |
| U1-SN (°) | 105.7 ± 6.3 | 103.4 | 114.0 | 108.5 | 112.4 |
| OP-SN (°) | 16.1 ± 5.0 | 16.8 | 14.5 | 14.8 | 17.5 |
| U1-L1 (°) | 124.2 ± 8.2 | 127.2 | 114.5 | 116.4 | 111.2 |
| Nasolabial angle (°) | 97.1 ± 10.7 | 102.9 | 100.7 | 103.5 | 99.4 |
| Lower lip to E-plane (mm) | 1.4 ± 1.9 | 0 | 1.5 | 1 | 1.5 |
Treatment objectives
Our objectives for this patient were to (1) eliminate dental crowding, and level and align the teeth, considering her main complaint; (2) obtain ideal overbite and overjet; (3) create a stable functional occlusion; (4) improve the mandibular midline shift; and (5) maintain a satisfactory soft-tissue profile.
Treatment objectives
Our objectives for this patient were to (1) eliminate dental crowding, and level and align the teeth, considering her main complaint; (2) obtain ideal overbite and overjet; (3) create a stable functional occlusion; (4) improve the mandibular midline shift; and (5) maintain a satisfactory soft-tissue profile.
Treatment alternatives
The main issue for this patient was the congenital absence of the 2 mandibular incisors. Based on the literature review, the following 3 options were proposed to the patient.
- 1.
Space expansion followed by restoration of the mandibular incisors with fixed dentures or implants. With this plan, an ideal Class I molar relationship and harmonized functional occlusion could be achieved. The disadvantages of this plan were the loss of healthy mandibular anterior teeth for fixed restoration or the presumed risks for implantation of mandibular incisors.
- 2.
Extraction of the maxillary second premolars and retraction of the maxillary incisors to obtain a Class II molar relationship. In this method, the maxillary canines would occlude with the mandibular first premolars. The disadvantages were the loss of 2 healthy premolars and the Bolton tooth-ratio problems.
- 3.
Anterior movement of the mandibular teeth to obtain ideal overjet and overbite. The adverse effect of this plan was that the occlusion would be settled in a new position and result in a Class III molar relationship after treatment.
After explaining the pros and cons of each alternative with the patient and her parents, they selected the third option for treatment.
Treatment progress
Treatment began with banding the first molars and bonding all other teeth (0.022 × 0.028-in edgewise appliance; Tomy, Tokyo, Japan). Tooth leveling and alignment were completed in 8 months by sequential changing of nickel-titanium wires. At the end of this phase, the anterior overjet was increased, and the molar relationship was still Class I ( Fig 4 ).

To prepare the teeth for Forsus FRD treatment, 0.019 × 0.025-in stainless steel wires were continually placed; for convenient use of the appliance, Ω loops were applied in the wires. Tight ligation from the mandibular left to the mandibular right first molars, rigid tieback of the arches, and cinchback of the wires were used to secure the mandibular arch position and to increase its anchorage. The Forsus FRD (32 mm) was assembled at chairside to push the mandible and the mandibular teeth forward. The mandibular teeth were moved forward, and the molars reached Class III relationships on both sides after the Forsus FRD was used for 6 months. At this stage, ideal anterior overbite and overjet were achieved. The midline remained unchanged ( Fig 5 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


