The Role of CAD/CAM in Modern Dentistry
Charles A.E. Slade
Principles
The processes of modern CAD/CAM dentistry can be broken down into several distinct phases, with the possibility of moving between digital and analogue workflows at several stages. Indeed, many dentists could be unaware that considerable aspects of their indirect restorations may be digitally produced already (Figure 6.9.1).
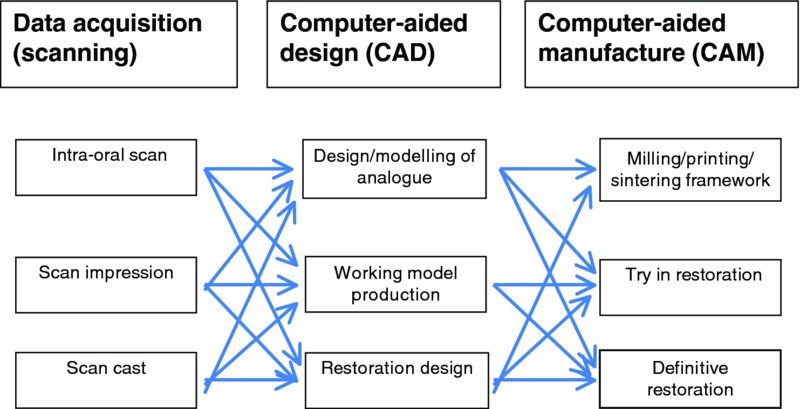
Figure 6.9.1 Phases of CAD/CAM dentistry
Data acquisition can be achieved directly from the patient or indirectly by scanning models or impressions. The goals for a successful scan are identical to those for an impression. It is essential to acquire an accurate copy of the teeth, tooth or implant being treated in addition to the surrounding tissue and adjacent teeth. Similarly, a representation of the remaining teeth in the arch, opposing surfaces and the dynamic interocclusal relationship between the opposing arches must also be recorded.
All scanners use a light source and a still or video camera or cameras to produce a digital image, in which the inherent accuracy of the image is a function of the accuracy of the camera, the speed of data acquisition and, significantly, the algorithm employed to model the data. In some systems a light powder, usually titanium oxide in a carrier medium, is applied to all the surfaces to be recorded to provide contrast or accurate reference points for the software to link the multiple images. Maintaining homogeneity and even thickness of this layer was a source of possible variation.1 The advent of powderless scanners has removed this source of inaccuracy with no limitation of scan accuracy,2 eliminating one of the main barriers to the technique. However, multiple reflective surfaces can still slow scan speeds significantly.
The three-dimensional (3D) image of any object is constructed of triangles, whose density of distribution is related to the density of the data present at any point on the object. You will notice in Figure 6.9.2 that the areas of low contour change are populated with sparse large triangles, while marginal areas show small, densely populated regions.
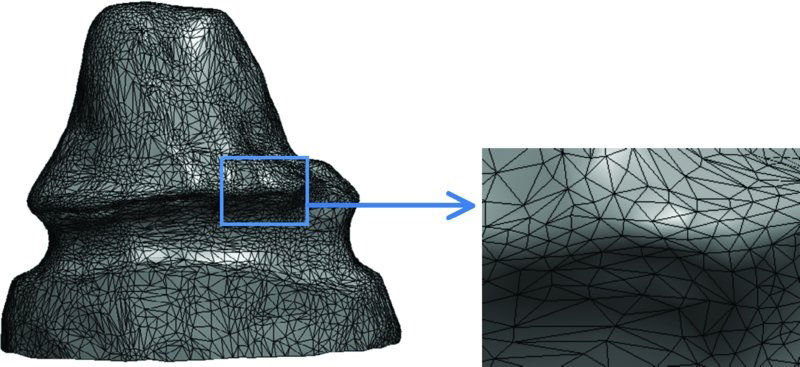
Figure 6.9.2 Triangulation and density distribution of data points across the varying surface of the preparation
These data sets create the 3D image, but also constitute a source of error, as there is a trade-off between accuracy and size of data file: doubling the data points and hence the accuracy quadruples the processing time. Files are stored and manipulated using Standard Tessellation Language, usually referred to as ‘STL’ files, which ideally are open source and directly available for manipulation without the need for third-party rendering.
These data files can be used to design and produce limited restorations ‘in house’ with chairside/bench-top milling machines and small furnaces, or sent to a remote laboratory where the restorations of a vast array can be designed and produced.
The software uses intelligent algorithms to create the scan and to some extent is capable of determining and correcting errors based on assumptions of the probable shapes of the missing data, as can be seen in Figure 6.9.3.

Figure 6.9.3 Actual scan data image (left) and image corrected with algorithm (right)
This and the inability of a digital scan to reproduce sharp angles absolutely (Figure 6.9.4) are limiting factors in scanning, and demand preparations to minimise these effects. The shape of the image being scanned is an approximation of the possible angular features of a dental preparation.
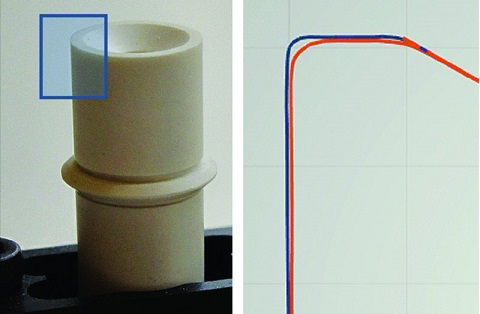
Figure 6.9.4 The two lines in the box on the right show the two-dimensional digital representation, by two scanners, of the surface marked by the box on the image on the left
More advanced programs remove unwanted soft-tissue incursion and highlight areas where greater data is required. Unlike an impression, this simply demands that the missing area be re-scanned, and the new data is overlaid and interlaced to the existing scan.
Despite this, the latest digital scanners are at least as accurate as a gold standard conventional impression3
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


