
Ensure Complete Bracket Engagement and Maintain Consolidation
New Approaches to Bracket Engagement
The very intriguing subjects of low-friction mechanics and self-ligating bracket systems have drawn much attention in the orthodontic profession. I try to keep an open mind to these treatment approaches; however, naturally my first thoughts are to compare this with the Alexander Discipline, which has evolved and been in use for more than 40 years. My conclusion is that treatment has been very successful with the existing methods involving the ligation of brackets, and I see no compelling reasons to change this approach, except possibly to improve efficiency with initial archwire ligation.
Low-friction ligation
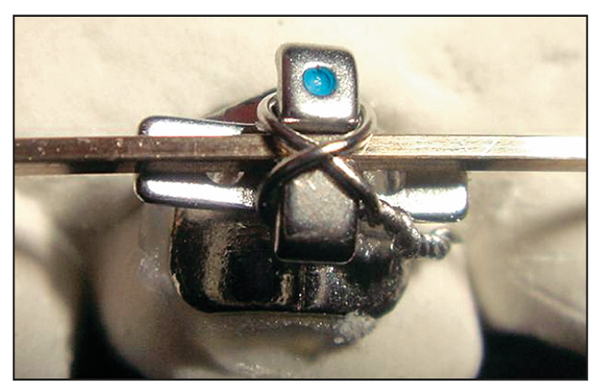
The potential advantages of low-friction ligation are found in the early stages of treatment during the initial alignment or “unraveling” of the anterior teeth, especially the maxillary anterior teeth. A special low-friction ligation technique —the figure-8 ligation (Fig 12-1)—is occasionally used in single brackets in the initial maxillary archwire with excellent results.
Self-ligation
The obvious advantage of a ligatureless bracket system is time savings. The reality is, however, that it is not possible to save time. It can only be used more efficiently. Removal and placement of archwires can often be accomplished faster with ligatureless brackets. However, some orthodontists have indicated that finishing proce dures are more difficult with the self-ligation appliances.
The question then becomes one of potential value. This question can only be answered by the individual clinician. My goal for an ideal bracket system would be one that is able to provide low friction early in treatment and three dimensional, high-friction control at the end of treatment. Three-dimensional control encompasses specific control of torques, angulations, and offsets. This subject will be explored further in future publications.
Traditional Archwire and Bracket Ligation
Elastomeric modules may be used to ligate initial archwires; however, early rotations are best ligated with steel ligatures to ensure better engagement in the bracket slot (Fig 12-2). All intermediate and finishing archwires are ligated with steel ligatures. When rectangular archwires are used, the wire should be completely engaged (with the archwire contacting the base of the slot). A torquing key may be used to accomplish this in certain situations (Fig 12-3).
Fig 12-2 Intraoral views of a patient with rotated teeth.

Figs 12-2a to 12-2c Pretreatment. Initial 0.016-inch nickel-titanium archwire with steel ligatures on rotated teeth and colored elastomers on nonrotated teeth.

Figs 12-2d to 12-2f Six weeks: Same patient.
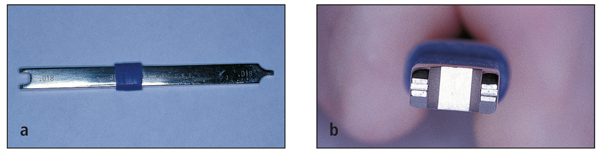
Figs 12-3a and 12-3b Although seldom needed, a torquing key can be used to help fully engage a 0.017 × 0.025-inch archwire in a 0.018-inch bracket slot.
Steel ligatures measuring 0.010 inch are used for tying rotations in flexible archwires and routine bracket engagement in other archwires. A 0.012-inch steel ligature wire is used to ligate difficult rotations, such as mandibular first molars, after conversion of the buccal tube. The 0.014-inch steel ligature wire is used for tying back.
The patient is told that he or she will experience some discomfort initially, but only for a short period.
Archwire Tieback to Maintain Consolidation
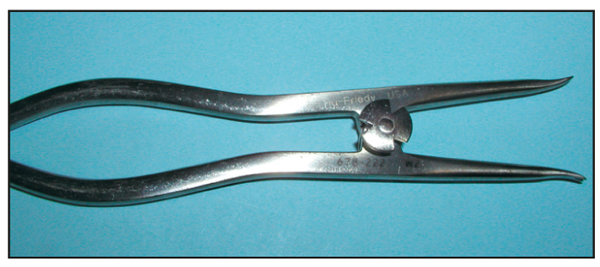
After spaces are closed, it is critical to maintain this arch consolidation. Various methods can be used to preserve arch integrity: continued use of elastomeric chains, fixation of teeth with ligature wire, or cinchback of the archwire distal to the terminal tubes. In the final analysis, the simplest and most reliable approach is to use omega loops mesial to the terminal tubes and to tie back with steel ligature wires using a special ligation-tying pliers (Fig 12-4).
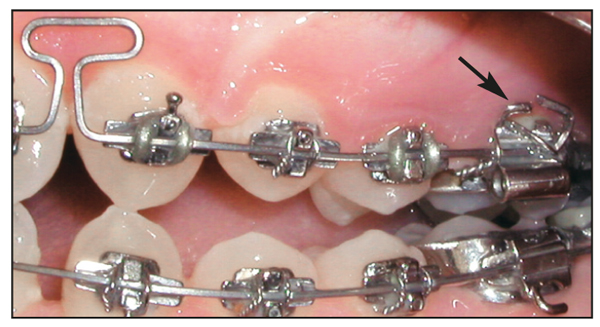
In extraction treatment, while closing loops are activated, the archwire can be cinched back distal to the first molars, assuming the second molars are not banded or bonded (Fig 12-5). When the second molars are banded, omega loops are placed just distal to the first molar bracket so that the closing loops are activated by tying back from the second molars (Fig 12-6).

Use of omega loops for tieback has several advantages:
- Active forces hold contact points together.
- Small spaces can be easily closed.
- It is unnecessary to change an elastomeric chain at each appointment.
- Spaces do not inadvertently open.
Rationale
Although it may not be necessary to tie back every archwire, the following side effects may occur if a tieback is not used:
- When an accentuated curve is placed in the max/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


