Establish Ideal Arch Form
For the first 20 years of my practice, all archwires were formed by hand from basic, single-sized arch “blanks.” These standard arch blanks were preformed from canineto-canine only and then extended posteriorly in a straight line, with no contours in the buccal segments. Each archwire was then individually adjusted to conform to the arch form desired for each patient.
In 1982, McKelvain1 reported on the measurement of 102 maxillary and mandibular, custom-formed, 0.017 × 0.025-inch stainless steel finishing archwires used in patients treated in my office. A composite arch form derived from the 102 custom-formed archwires was created and manufactured beginning in 1984. This template has been used in our office ever since (Fig 9-1).
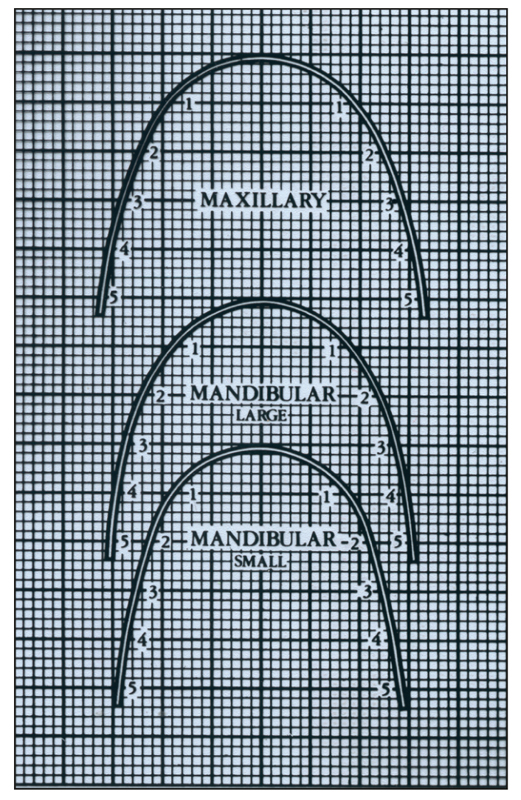
Fig 9-1 Alexander arch form template. This maxillary arch form is used on every patient. It may be expanded or constricted if needed, usually within one standard deviation. The template has two mandibular arch forms. The intercanine width is the same in both arch forms; the difference between them is the posterior width.
The research on mandibular arch forms by Felton et al2 is considered a landmark study on the subject. When 17 commercially available arch form templates were compared, it was determined that 50% of the arch forms studied approximated those of the Vari-Simplex Discipline (Ormco). However, “changes in arch form with treatment frequently were not stable; almost 70% of cases (30 Class I and 30 Class II, nonextraction cases) showed significant long-term posttreatment changes.”2
An arch form study by Lapointe et al,3 using patient records from my office, concluded that, “the orthodontist has only a limited influence on arch form during and after treatment.” These cases were all Class I, extraction and nonextraction. No expansion therapy was used on any patient. These 39 patients had been out of treatment an average of 15 years.
Determination of the Ideal Arch Form
Based on the studies of patients treated in my office1 and the long-term stability of these cases, I have come to the following conclusions about ideal arch form.
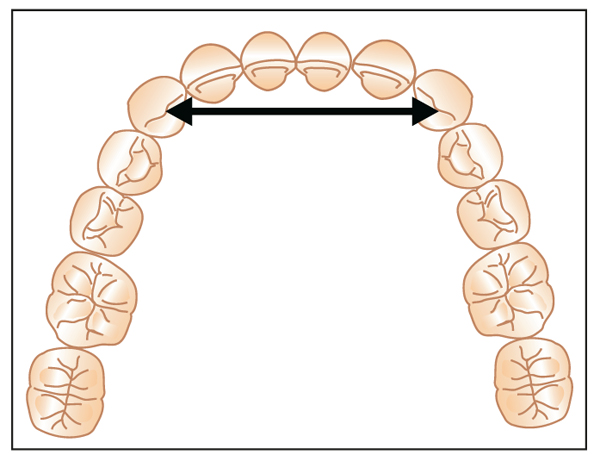
First, the anterior segment of any arch form should be dictated by the mandibular intercanine width (Fig 9-2) and the position of the mandibular incisors (Fig 9-3). Unless the canines have erupted abnormally lingually, the intercanine width should be expanded less than 1 mm.
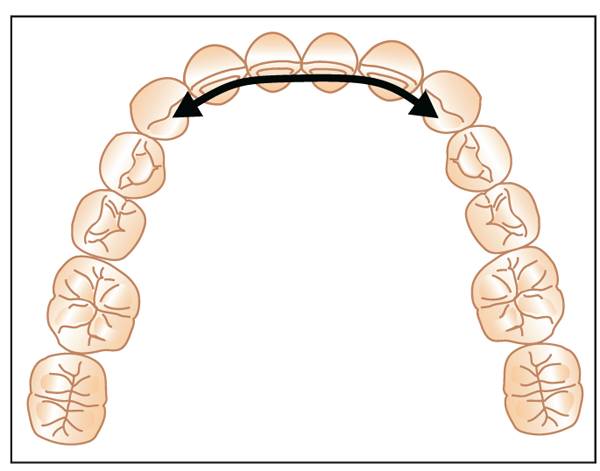
Second, the mandibular incisors should be kept in an upright position. This anterior segment of the mandibular arch form was taught by Tweed with the Bonwell-Hawley arch form. Because little variation in arch form can take place in the mandibular anterior segment, the maxillary anterior arch form, from canine to canine, must then conform to the mandibular arch form (Fig 9-4).
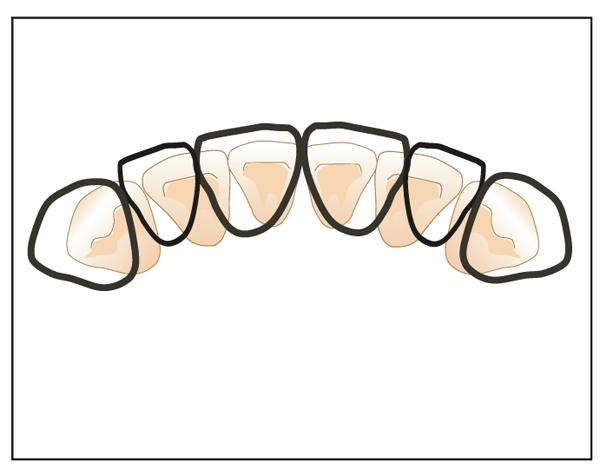
Fig 9-4 The arch form of the maxillary anterior teeth is dictated by the configuration of the mandibular canine-to-canine relationships.
Third, the final shape of the posterior segments of the maxillary arch form is dictated by the maxillary intermolar width. Studies4,5 have shown that the long-term posttreatment maxillary intermolar width, after nonextraction therapy, averages around 35 to 37 mm. This is measured at the lingual central groove of the maxillary first molars, at the cervical line (Fig 9-5). The posterior segments of the Alexander Discipline arch form are thus designed to conform to this width (Fig 9-6).
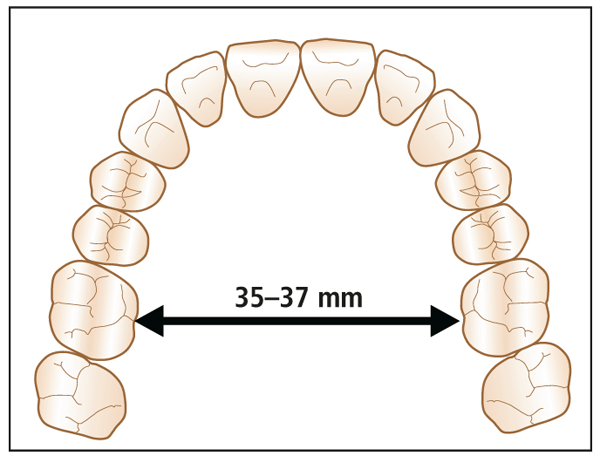
Fig 9-5 Maxillary intermolar width determines the final arch form. Using this technique to create the final arch form will always produce an ovoid shape.
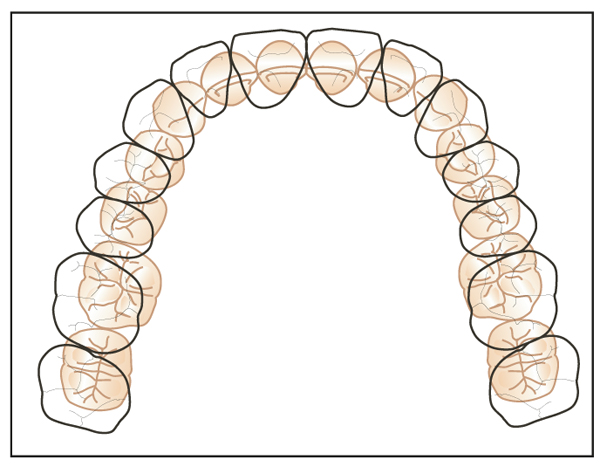
Fig 9-6 The mandibular posterior arch can then be expanded or constricted to occlude properly with the maxillary arch.
Clinical Arch Form Adjustments
In most cases, the maxillary arch is treated prior to the mandibular arch. The untreated mandibular arch then serves as the guide while the maxillary arch is finalized with a 0.017 × 0.025-inch stainless steel archwire. Later in treatment, the treated maxillary arch serves as the guide to coordinate the two arches when the 0.017 × 0.025-inch stainless steel mandibular arch is formed.
Clinically, the final maxillary arch form (0.017 inch stainless steel archwire) is customized by observing the patient’s buccal overjet when the mandible is positioned forward into a Class I relationship (Fig 9-7). The arch form is then expanded or constricted in the posterior region to create the ideal buccal overjet exhibited in the protruded Class I position (Fig 9-8).

Fig 9-7 (a) Maxillary arch ready for 0.017 × 0.025-inch SS final arch.(b) Mandible positioned forward into final Class I relationship to observe buccal overjet. (c) Observe need for maxillary posterior expansion to create normal buccal overjet.

Fig 9-8 (a) Maxillary 0.017 × 0.025-inch SS archwire placed in anterior brackets. (b) Archwire expanded in buccal segments. (c) Final occlusion before bracket removal.
When the final mandibular arch form is placed with the 0.017 × 0.025-inch stainless steel archwire, the original intercanine width is checked. The patient is then asked to protrude the mandible into an ideal overbite, overjet, and Class I occlus/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


