The patient was a 16-year-old Japanese girl whose chief complaints were crowding and transposition of the maxillary canine and first premolar. A setup model was used to preoperatively align the teeth in their transposed positions. The amount of postoperative reshaping was estimated for the occlusal surfaces of the teeth. However, the patient did not wish to have her teeth reduced by reshaping or to have composite materials for restorative camouflage. Because she strongly expected alignment of her teeth in the correct intra-arch position, her transposed teeth were corrected without extraction of the transposed teeth. Cone-beam computed tomography was used to obtain more detailed information about the transposition, and the direction of tooth movement was examined. Although the duration of the treatment was long, both the crowns and the roots of the transposed teeth were aligned correctly.
Transposition of teeth is defined as an interchange of position of 2 teeth in the dental arch, and its incidence is relatively rare. The maxillary canine and first premolar transposition is most frequently described in the literature, followed by transposition of the maxillary lateral incisor with the canine. Unilateral transpositions have been reported more often than bilateral transpositions, and the left side has been more frequently involved than the right. Transposition can be complete or incomplete. In a complete transposition, both the crowns and the entire root structures of the involved teeth are found in their transposed positions. In an incomplete transposition, the crowns might be transposed, but the root apices still remain in their normal positions. Several factors should be considered when making an orthodontic treatment plan for transposed teeth. In extraction treatment, many patients are treated by extraction of either tooth. In nonextraction treatment, patients undergo alignment of teeth in their normal positions or in their transposed positions. Whichever treatment is selected, several factors (positions of the crowns and roots, gingivae of the transposed teeth, caries risk, and duration of treatment) should be considered when making an orthodontic treatment plan for transposed teeth. This case report demonstrates the successful alignment of a complete maxillary canine and first premolar transposition in their normal positions with nonextraction treatment. Good results have been maintained for 2 years after active orthodontic treatment.
Diagnosis and etiology
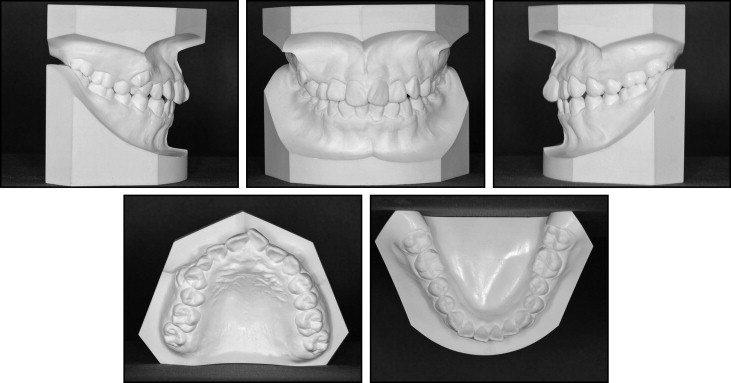
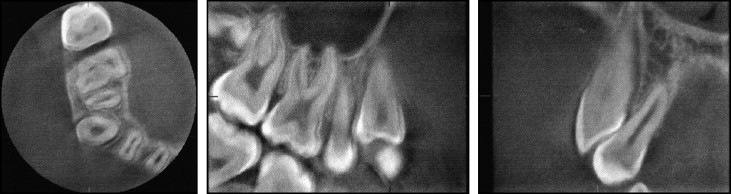
The patient was a 16-year-old Japanese girl. Her chief complaints were crowding and transposition of the maxillary right canine and first premolar. She had no orthodontic history. The pretreatment facial photographs showed a symmetric facial pattern with a straight profile ( Fig 1 ). The intraoral examination showed an Angle Class III molar relationship bilaterally. All permanent teeth were erupted, and the maxillary right deciduous canine was retained. The maxillary right permanent canine had erupted in an ectopic position between the 2 premolars. The maxillary right first premolar was in scissorsbite. The arch length discrepancies were –4.3 mm in the maxillary arch and –1.9 mm in the mandibular arch. She had +3.0 mm of overjet and +2.0 mm of overbite. Both maxillary and mandibular dental midlines nearly coincided with the facial midline ( Figs 1 and 2 ). On radiographic examination, the root of the maxillary right deciduous canine was mostly resorbed, and both the crowns and the roots were transposed ( Fig 3 ). Dental computed tomography scans showed that the root of the right canine was between the premolars, and the root of the first premolar was close to the crown of the canine but not resorbed ( Fig 4 ). Maxillary canine and first premolar transposition is the most frequent type of transposition. Several etiologies of transposition have been proposed: genetic origin, trauma, interchange of the position of the developing tooth buds, lack of deciduous canine root resorption, early loss of deciduous teeth, and prolonged retention of deciduous teeth. Because of the high incidence of retained deciduous canines associated with tooth transpositions, some authors have reported that deciduous teeth are the primary etiologic factor of this anomaly. In this patient, a possible etiology of transposition included the retained deciduous canine. In the lateral cephalometric radiograph, the maxilla was positioned posteriorly, and the mandible was positioned normally relative to Japanese standards (SNA, 78.2°; SNB, 76.7°; ANB, 1.5°). The patient had a skeletal Class III relationship. The inclination of the maxillary incisors was normal, but the mandibular incisors showed a lingual inclination ( Fig 5 , Table ). From these findings, the patient was diagnosed with an Angle Class III malocclusion with crowding and transposition of the maxillary right canine and first premolar.



| Measurement | Mean | SD | Pretreatment | Posttreatment | Two years posttreatment |
|---|---|---|---|---|---|
| SNA (°) | 82.3 | 3.5 | 77.5 | 78.0 | 78.0 |
| SNB (°) | 78.9 | 3.5 | 76.0 | 75.1 | 75.2 |
| ANB (°) | 3.4 | 1.8 | 1.5 | 2.9 | 2.8 |
| FMA (°) | 28.8 | 5.2 | 29.7 | 30.6 | 30.6 |
| Gonial angle (°) | 122.2 | 4.6 | 125.8 | 123.3 | 123.3 |
| Ramus inclination (°) | 2.9 | 4.4 | 6.1 | 2.7 | 2.7 |
| Occlusal plane to FH (°) | 11.4 | 3.6 | 10.2 | 15.9 | 15.5 |
| U1 to SN (°) | 104.5 | 5.6 | 111.1 | 97.3 | 98.0 |
| FMIA (°) | 58.0 | 66.8 | 59.4 | 60.2 |
Treatment objectives
The treatment objectives were to correct the transposition, establish the natural tooth order by extraction of the maxillary right deciduous canine without extraction of the transposed tooth, establish a functional Class I molar and canine relationship with coincident dental midlines, create ideal overbite and overjet, and correct the lingual inclination of the incisor.
Treatment objectives
The treatment objectives were to correct the transposition, establish the natural tooth order by extraction of the maxillary right deciduous canine without extraction of the transposed tooth, establish a functional Class I molar and canine relationship with coincident dental midlines, create ideal overbite and overjet, and correct the lingual inclination of the incisor.
Treatment alternatives
The following alternatives were considered for the transposed teeth: (1) extraction of all first premolars, (2) extraction of the maxillary right canine or first premolar, (3) nonextraction treatment and alignment of the teeth in the transposed order, and (4) nonextraction treatment and correction of the transposition.
In considering these treatment alternatives, the following factors were taken into account. Because the facial appearance was satisfactory for a Japanese girl, she did not need retraction of the lips. Treatment with extraction of the 4 first premolars would have required extensive linguoclination of the maxillary and mandibular incisors, or it would have required extensive mesial movement of the molars.
In addition, if either the maxillary right first premolar or the canine had been extracted, that dental arch would have become asymmetric, and the treatment mechanics would have become difficult. Therefore, we evaluated how the transposed teeth could be aligned without tooth extractions. Because both the crown and the root were transposed in the maxillary right first premolar and canine, aligning the teeth in the transposed order would probably have required a shorter treatment time than correcting the transposition. Correction of a transposition poses a high risk of damaging the teeth or the supporting structures. Thus, alignment of the involved teeth in their transposed positions seemed to be the best alternative, but the patient strongly desired alignment of the teeth in their correct positions. Dental computed tomography showed that the roots of the transposed teeth were in close proximity, but root resorption was not observed. From a diagnostic setup model ( Fig 6 ), if the teeth were to have been aligned in their transposed positions, extensive reshaping and camouflage restoration might have been required. We decided to attempt treatment without extraction of the transposed tooth and with correction of the transposition to achieve a functional Class I canine and molar relationship.


