The purpose of orthodontic treatment is to prevent and improve functional malocclusion so that comprehensive and effective masticatory function can be established. The physiological importance of the stomatognathic system is indispensable for normal structure and function. Studies have shown that malocclusion patients have lower masticatory function than patients with normal occlusion, resulting in a general decrease in oral function caused by occlusal disharmony, less occlusal force and chewing ability, and other issues. The reasons why subjects with malocclusion have poorer masticatory performance are not completely understood. However, three factors that might influence masticatory performance are (1) the number and area of occlusal contacts, (2) occlusal forces as reflected by maximum bite force, and (3) the amount of lateral excursion during mastication. Masticatory function can be improved by orthodontic treatment, but it is extremely difficult to measure the degree of improvement.
To better evaluate the effectiveness of treatment, the focus of diagnosis should be more on occlusal force and occlusal contacts. The investigation of occlusal force began with Borelli’s mandibular force meter in 1681 and was followed by various other studies. The predominant methods for measuring occlusal force are (1) cantilever, (2) oil pressure, (3) Brinnel hardness, (4) electricity, (5) T-scan, and (6) Prescale. Dahlberg reported that there are 32 points of occlusal contact area (26 in molar region). Hellman measured the contact areas at centric occlusion and described 138 contact points in an ideal occlusion by classifying (1) the contact condition, (2) the contact with cusp and fissure, (3) the contact with marginal ridge and interdental embrasure, and (4) the contact with marginal ridge and fissure.
A recent shift in the interpretation of occlusal force has resulted from the “T-scan” system and its use with image-analysis technology. The T-scan system is an occlusal measuring device that was created by Maness et al. in 1987. Its primary application is in measuring the differences in electrical resistance, which is representative of occlusal force. However, Patyk et al. reported that the sensor of the T-scan system is thick and tends to dislocate the mandible because of the inherent flexibility in the system. Also, the T-scan system has a narrow measurement range for occlusal force, as well as varying sensitivity at different measurement locations within that range. However, the recent development of the Dental Prescale Occluzer System (Fuji Film, Tokyo, Japan) allows for easy measurements of occlusal contact areas and pressures in occlusion. This system is used widely in Japanese orthodontics. Uchiyama et al. confirmed a high rate of reproduction and reliability in the occlusal contact area measurement taken by this system. Nagai et al. reported that pressure-sensitive sheets are useful in the study of occlusal status of mandibular prognathism. Also, Asano et al. obtained reliable results using the system when examining the change in occlusal force and contact areas during retention.
This chapter addresses the evaluation of occlusal patterns, especially occlusal contact areas and pressures in orthodontic patients, using the Dental Prescale Occluzer System.
DENTAL PRESCALE OCCLUZER SYSTEM
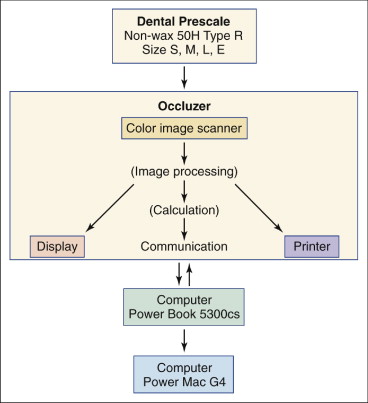
The Dental Prescale Occluzer System consists of pressure-sensitive sheets (Dental Prescale), an analyzing computer (Occluzer), and a data-saving computer (Macintosh Power Book) ( Figs. 4-1 and 4-2 ). The density of color formation on the pressure-sensitive sheets depends on the level of pressure applied. The color formations on the sheets are read by the Occluzer with a color-imaging scanner. The magnitude of occlusal pressure and force is estimated by examining the identified color density and area data.
Prescale Sheet Design
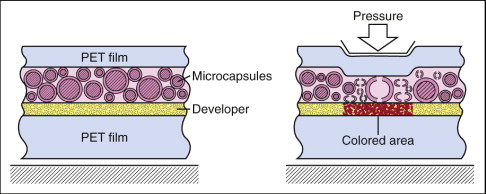
The Dental Prescale incorporates a monosheet design. First, a developer solution is coated over a base layer of polyethylene terephthalate (PET) film. Microcapsules of various dimensions that contain color former are uniformly distributed across this developer layer. Both sides are then vacuum-wrapped in an ultrathin layer of PET film. Special measures are taken throughout the manufacturing process to ensure that each Dental Prescale sheet is completely sterile.
When the Prescale sheet is subjected to pressure, the microcapsules break and release a colorless, clear leuco (white) dye. This dye reacts with the developer layer and turns red. Because the microcapsules can withstand various pressures, depending on their size and thickness, the shade and intensity of the dye will vary with the amount of pressure applied to the Prescale sheet; greater pressure yields deeper color. Large and thin microcapsules break when subjected to relatively low pressure, whereas small and thick microcapsules only break when subjected to greater pressure. The shade of red produced darkens in proportion to the number of capsules that break.
Occlusal Force Measuring System
The Occluzer FPD-703 (Fuji Film), an occlusal force measuring system, consists of a scanner, treating board, monitor, thermal printer, and mouse. Measuring begins when the Prescale image is scanned into the computer. The computer then reads the color formation (information provided by Prescale) at 100 dots per inch (dpi) and identifies data with the treating board. The process is completed when the information is expressed in analog data form.
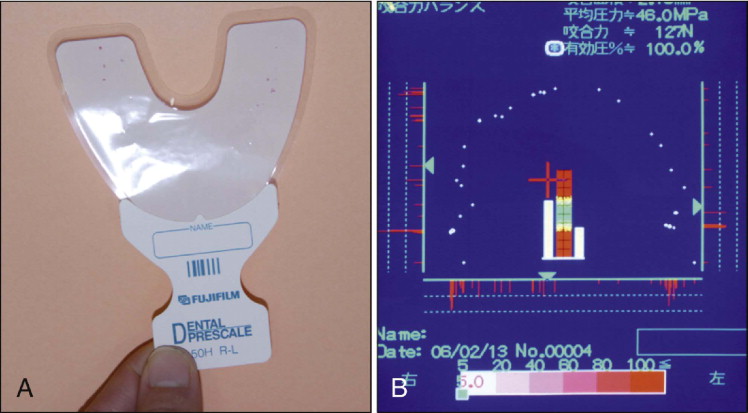
The Dental Prescale 50H Type R (Fuji Film) used in this study is horseshoe shaped so that it fits on the dental arch. There are four sizes available: S, M, L, and E.
In previous studies, modeling compounds, a shellac bite plate, and a silicone block were used to mark the occlusal contacts. The Dental Prescale is more precise and convenient than these methods. Type R is more precise and thicker than Type W. Moreover, only the contact area between upper and lower teeth is marked in Type R.
Analysis
Analyzing the results of the Dental Prescale involves the following measurements:
- •
Occlusal contact area (“Area”) is the area color-formatted by the Prescale. Low occlusal forces cannot be calculated under the measuring range of the Prescale. The units are given in square millimeters (mm 2 ).
- •
Average occlusal pressure (“Average” [“Ave”]) is the occlusal force per unit area, expressed in megapascals (MPa).
- •
Occlusal force (“Force”). is calculated by multiplying average occlusal pressure and occlusal contact area. The units are given in newtons (N); 1 N ≅ 0.1 kilogram-force (kgf).
When using the Dental Prescale, the subject sits in the dental chair in a relaxed position. After a “warm-up” that consists of mild to strong biting two or three times, the patient is directed to bite the Prescale sheet ( Fig. 4-3, A ) only once and hold the bite for 5 seconds. The Prescale sheet is then inserted into the Occluzer to analyze the data (Macintosh Power Book5300cs, Power Mac G4), the occlusal contact areas (mm 2 ), pressure on each occlusal contact area (MPa), and all the occlusal forces (N) ( Fig. 4-3, B ).
CLINICAL STUDY
Subjects
In this clinical study, subjects with different malocclusions and various facial patterns were selected from incoming patients at the Kitafusa Orthodontic Clinic (Asahi, Chiba, Japan). Subjects with normal occlusion were chosen from office staff and their friends. These subjects had no missing or decayed teeth and had not undergone any orthodontic or prosthodontic treatment. The normal-occlusion subjects displayed a Class I molar relationship, as defined by Angle classification.
Normal-occlusion and malocclusion subjects were distributed as shown in Table 4-1 . Subjects with maxillary protrusion were classified into two types: those with greater than 5 mm of overbite (“ov” [over] type), and those with less than 5 mm of overbite (“un” [under] type). Cephalometric analyses were done for all the patients ( Table 4-2 ). Facial angles measured were facial axis (FX), facial depth (FD), mandibular plane (MP), and mandibular arc (MA). Lower facial height (LFH) and total facial height (TFH) were also measured). Facial patterns were classified according to the Ricketts method ( Table 4-3 ) and analyzed cephalometrically ( Table 4-4 ).
| Normal/Malocclusion | Number | Average Age |
|---|---|---|
| Normal occlusion | 10 | 14.10 ± 4.27 |
| Crowding | 21 | 12.73 ± 7.12 |
| Mandibular protrusion | 19 | 10.96 ± 4.27 |
| Maxillary protrusion (ov) | 18 | 12.79 ± 5.52 |
| Maxillary protrusion (un) | 10 | 14.21 ± 7.63 |
| Lateral crossbite | 5 | 13.20 ± 7.10 |
| Open bite | 20 | 12.51 ± 5.25 |
| total | 103 | 12.93 ± 7.30 |
| Normal/Malocclusion | FX | FD | MP | LFH | MA | TFH |
|---|---|---|---|---|---|---|
| Normal occlusion | 86.52 ± 2.98 | 84.30 ± 3.43 | 29.64 ± 3.62 | 46.44 ± 1.50 | 31.82 ± 4.81 | 58.50 ± 2.11 |
| Crowding | 84.46 ± 4.25 | 84.41 ± 3.05 | 32.39 ± 4.66 | 48.22 ± 4.17 | 33.30 ± 4.18 | 61.14 ± 4.56 |
| Mandibular protrusion | 89.24 ± 3.23 | 87.60 ± 4.27 | 28.39 ± 5.99 | 44.67 ± 4.08 | 33.80 ± 6.96 | 57.32 ± 4.58 |
| Maxillary protrusion (ov) | 83.84 ± 2.54 | 83.46 ± 2.55 | 31.43 ± 3.10 | 46.30 ± 3.32 | 34.88 ± 2.64 | 58.72 ± 3.49 |
| Maxillary protrusion (un) | 85.34 ± 3.75 | 85.28 ± 2.20 | 31.66 ± 4.55 | 45.03 ± 3.80 | 31.53 ± 4.98 | 59.93 ± 4.23 |
| Lateral crossbite | 83.12 ± 5.49 | 85.46 ± 2.74 | 34.54 ± 4.41 | 49.68 ± 5.06 | 29.18 ± 6.63 | 65.20 ± 4.85 |
| Open bite | 83.26 ± 5.55 | 85.45 ± 3.26 | 33.70 ± 5.87 | 51.47 ± 5.88 | 31.00 ± 4.58 | 64.09 ± 6.04 |
| Pattern | Number | Average Age |
|---|---|---|
| Severe dolichofacial | 17 | 13.23 ± 2.77 |
| Dolichofacial (dolicho) | 19 | 12.25 ± 3.70 |
| Mesiofacial, tendency to dolichofacial | 17 | 13.37 ± 8.23 |
| Mesiofacial (mesio) | 19 | 11.38 ± 6.51 |
| Mesiofacial, tendency to brachyfacial | 22 | 11.33 ± 4.74 |
| Brachyfacial (brachy) | 13 | 12.45 ± 6.99 |
| Severe brachyfacial | 17 | 12.44 ± 4.81 |
| total | 124 | 12.35 ± 5.39 |
| Pattern | FX | FD | MP | LFH | MA | TFH |
|---|---|---|---|---|---|---|
| Severe dolichofacial | 82.64 ± 5.74 | 84.17 ± 3.03 | 35.40 ± 5.98 | 50.60 ± 6.72 | 30.86 ± 5.47 | 63.97 ± 7.09 |
| Dolichofacial (dolicho) | 84.91 ± 3.70 | 84.09 ± 2.79 | 33.11 ± 4.54 | 48.46 ± 4.31 | 31.41 ± 4.10 | 60.69 ± 4.31 |
| Mesio, tendency to dolicho | 83.22 ± 4.08 | 83.74 ± 2.82 | 34.52 ± 4.25 | 49.08 ± 3.19 | 31.57 ± 4.80 | 62.79 ± 4.74 |
| Mesiofacial (mesio) | 83.66 ± 3.22 | 83.64 ± 2.45 | 32.88 ± 2.94 | 47.87 ± 3.93 | 29.86 ± 4.86 | 62.64 ± 3.50 |
| Mesio, tendency to brachy | 87.45 ± 2.88 | 87.26 ± 3.74 | 29.79 ± 2.99 | 46.20 ± 1.99 | 32.11 ± 4.30 | 59.33 ± 2.78 |
| Brachyfacial (brachy) | 86.47 ± 2.96 | 85.58 ± 2.64 | 29.09 ± 3.13 | 45.73 ± 3.23 | 34.37 ± 3.24 | 58.37 ± 3.11 |
| Severe brachyfacial | 90.72 ± 3.30 | 88.67 ± 3.06 | 24.95 ± 3.49 | 41.05 ± 2.33 | 38.74 ± 3.48 | 53.73 ± 2.38 |
Methods
Biting force was recorded for subjects with normal occlusion, subjects with various malocclusions, and subjects representing the seven facial patterns using the pressure-sensitive sheets (Dental Prescale 50H Type R). The data obtained were classified for each group, and statistical analysis was performed using Microsoft Excel 8.0. Data from each group of normal-occlusion and malocclusion subjects and facial pattern subjects were tested by the Stat-View J 5.0. One-way Factorial Analysis of Variance (ANOVA) and Multiple Comparison tests and the Scheffe method were used later to determine significant differences among groups.
Results
The occlusal patterns in subjects with normal occlusion and in those with malocclusions were analyzed. Table 4-5 and Figure 4-4 shows the average value of occlusal contact areas (“Area”), average occlusal pressure on occlusal contacts (“Average”/“Ave”), and all the occlusal force (“Force” = “Ave” × “Area”). The results are as follows:
- 1.
Normal-occlusion group. Values of “Area” and “Force” were highest when compared with each malocclusion group. However, “Average” was not significantly higher but rather was similar to the average values.
- 2.
Mandibular protrusion group. Despite values of “Average” being the lowest, “Area” was the highest in the mandibular protrusion group after the normal-occlusion group. “Force” also was highest in this group after the normal-occlusion group.
- 3.
Crowding group. “Area” and “Force” showed high values in the crowding malocclusion group similar to the mandibular protrusion group. “Average” was lowest, after the mandibular protrusion group.
- 4.
Maxillary protrusion group. In “Area” and “Force” the maxillary protrusion (“un”) and maxillary protrusion (“ov”) groups had significantly different values. The “un” was near average in all groups and was higher than “ov” in “Area” and “Force.” However, the “Average” for “ov” was near average and higher than for “un.”
- 5.
Lateral crossbite group. “Average” was highest after the normal-occlusion group, and “Area” and “Force” were second lowest in value.
- 6.
Open-bite group. “Area” and “Force” were lowest in all subject groups; however, “Average” was highest in all groups.
| Normal/Malocclusion | C ontact A rea ( mm 2 ) | P ressure (MP a ) | O cclusal F orce (N) | |||
|---|---|---|---|---|---|---|
| Average | SD | Average | SD | Average | SD | |
| Normal occlusion | 8.48 | 2.67 | 51.09 | 7.71 | 423.27 | 113.92 |
| Mandibular protrusion | 7.60 | 3.80 | 46.13 | 6.79 | 348.91 | 172.02 |
| Crowding | 7.49 | 3.58 | 46.95 | 5.39 | 346.10 | 154.16 |
| Maxillary protrusion (un) | 6.04 | 3.12 | 47.22 | 5.32 | 281.46 | 141.22 |
| Lateral crossbite | 4.80 | 1.80 | 51.12 | 10.28 | 245.62 | 104.22 |
| Maxillary protrusion (ov) | 4.70 | 3.25 | 50.14 | 8.80 | 222.37 | 146.79 |
| Open bite | 3.33 | 1.36 | 52.16 | 6.02 | 170.92 | 68.74 |
| average | 5.64 | 2.11 | 50.03 | 3.12 | 273.32 | 94.97 |
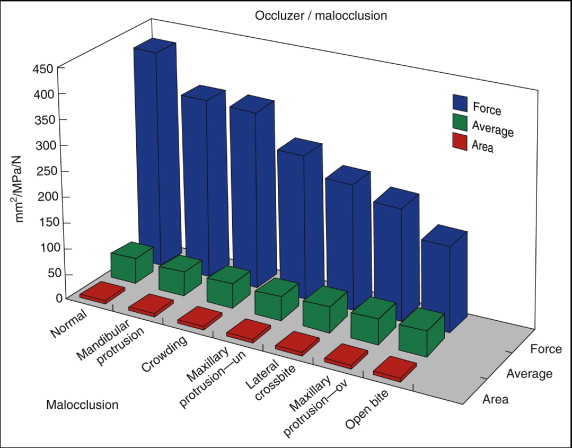
To summarize the results, force decreased in the following order: normal occlusion, mandibular protrusion, crowding, maxillary protrusion (un), lateral crossbite, maxillary protrusion (ov), and open bite.
Table 4-6 lists the statistical data for the significant differences among normal-occlusion and malocclusion groups. Within occlusal contact area, normal occlusion vs. open bite, crowding vs. open bite, and mandibular protrusion vs. open bite displayed significant differences. Within average pressure, no significant differences were recognized. Within occlusal force, normal occlusion vs. maxillary protrusion (ov), normal occlusion vs. open bite, crowding vs. open bite, and mandibular protrusion vs. open bite, there were significant differences.
| C ontact A rea | A verage P ressure | O cclusal F orce | ||||
|---|---|---|---|---|---|---|
| p | p | p | ||||
| Normal/crowding | 0.9944 | 0.8777 | 0.9123 | |||
| Normal/mandibular protrusion | 0.9967 | 0.7227 | 0.9159 | |||
| Normal/maxillary protrusion (ov) | 0.1527 | >0.9999 | 0.0450 | * | ||
| Normal/maxillary protrusion (un) | 0.7239 | 0.9328 | 0.4212 | |||
| Normal/lateral crossbite | 0.5801 | >0.9999 | 0.4921 | |||
| Normal/open bite | 0.0080 | † | >0.9999 | 0.0024 | † | |
| Crowding/mandibular protrusion | >0.9999 | >0.9999 | >0.9999 | |||
| Crowding/maxillary protrusion (ov) | 0.2710 | 0.9152 | 0.2863 | |||
| Crowding/maxillary protrusion (un) | 0.9354 | >0.9999 | 0.9371 | |||
| Crowding/lateral crossbite | 0.8041 | 0.9610 | 0.9093 | |||
| Crowding/open bite | 0.0093 | † | 0.4643 | 0.0197 | * | |
| Mandibular protrusion/maxillary protrusion (ov) | 0.1811 | 0.7444 | 0.2123 | |||
| Mandibular protrusion/maxillary protrusion (un) | 0.8926 | 0.9998 | 0.9101 | |||
| Mandibular protrusion/lateral crossbite | 0.7554 | 0.9018 | 0.8896 | |||
| Mandibular protrusion/open bite | 0.0036 | † | 0.2264 | 0.0099 | † | |
| Maxillary protrusion (ov)/maxillary protrusion (un) | 0.9597 | 0.9640 | 0.9633 | |||
| Maxillary protrusion (ov)/lateral crossbite | >0.9999 | >0.9999 | >0.9999 | |||
| Maxillary protrusion (ov)/open bite | 0.9307 | 0.9916 | 0.9708 | |||
| Maxillary protrusion (un)/lateral crossbite | 0.9963 | 0.9773 | 0.9997 | |||
| Maxillary protrusion (un)/open bite | 0.3942 | 0.6491 | 0.5206 | |||
| Lateral crossbite/open bite | 0.9886 | >0.9999 | 0.9783 | |||
Table 4-7 and Figure 4-5 show the average values of “Area,” “Average,” and “Force” among the different facial pattern groups, as follows:
- 1.
Severe dolichofacial (dolicho) pattern. “Area” and “Force” were the lowest of all groups. “Average” was slightly higher than the average value.
- 2.
Dolichofacial pattern (“dolicho”). This type of pattern showed second lowest on “Area” and “Force”. “Average” showed the highest in all groups.
- 3.
Mesiofacial (mesio) pattern tendency to dolichofacial. “Area” and “Force” showed third lowest. “Average” showed almost the same as severe dolichofacial pattern.
- 4.
Mesiofacial pattern. “Area”, “Average”, and “Force” were midway between the high and low positions.
- 5.
Mesiofacial pattern tendency to brachyfacial (brachy). “Area” and “Force” were the third highest of all groups. “Average” was almost near to average values.
- 6.
Brachyfacial pattern (“brachy”). “Area” was almost the same as the severe brachy pattern, but was the highest value of all groups. “Average” was the lowest of all groups, and “Force” was second highest.
- 7.
Severe brachyfacial pattern. “Force” was the highest of all groups. “Area” was nearly as high as brachyfacial pattern. “Average” was close to average.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


