One of the major concepts that has emerged during the author’s 40+ years of clinical practice in orthodontics concerns the diagnosis and treatment of what can be termed maxillary deficiency syndrome. In fact, maxillary transverse and/or sagittal deficiency may be one of the most pervasive skeletal problems in the craniofacial region, especially in patients of European ancestry. Many of the individual characteristics or symptoms of this condition have been well recognized in orthodontics, but rarely are they combined conceptually. However, it may be possible to produce a greater treatment effect on the skeletal structures of the maxillary complex than in the mandible, particularly with regard to the management of the transverse dimension.
MANIFESTATIONS OF MAXILLARY TRANSVERSE DEFICIENCY
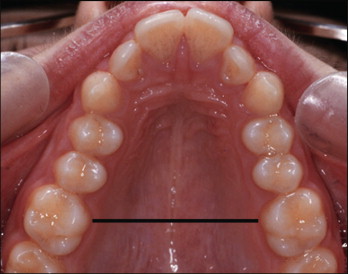
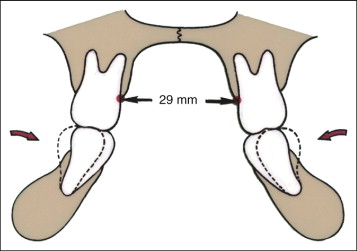
The manifestations of maxillary transverse deficiency are encountered by the orthodontist on a daily basis, but usually they are not quantified. As part of an initial evaluation of a patient, it is recommended that the distance between the closest points of the maxillary first molars (i.e., transpalatal width ) be measured ( Fig. 12-1 ). Typically, a maxillary arch with a transpalatal width of 35 to 39 mm can accommodate a dentition of average size without crowding or spacing. However, maxillary arches less than 31 mm in transpalatal width may be crowded and thus in need of orthopedic expansion in growing individuals or surgically assisted expansion in adults. Other factors that must be considered when making the extraction/expansion decision include facial type, soft tissue profile, and level of muscle tonus.
Transverse Skeletal Imbalances
A major conceptual leap is from using rapid maxillary expansion (RME) in the correction of posterior crossbite to using RME in patients without crossbite. Orthodontists traditionally have used RME to correct posterior crossbites, but little else. In contrast to the aggressive approaches often taken in treating skeletally based anteroposterior and vertical problems, many orthodontists have been reluctant to change arch dimensions transversely. However, the transverse dimension of the maxilla may be the most adaptable of all the regions of the craniofacial complex. Many, if not most, transverse skeletal imbalances in the maxilla are ignored or simply not recognized, and thus the treatment options for such patients are necessarily more limited than if these imbalances were considered.
Crowding and Protrusion
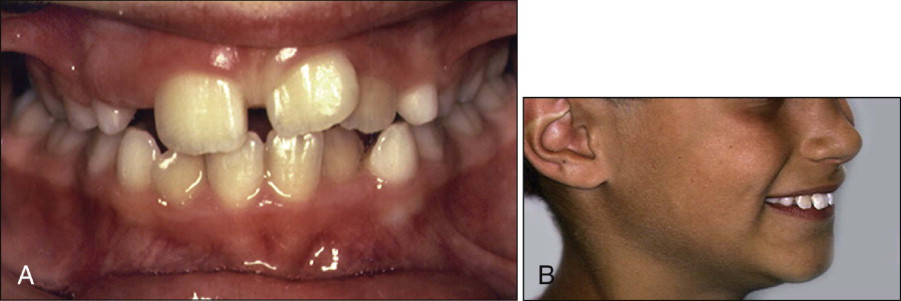
Other than crossbite, two of the most common problems encountered by the orthodontist are crowding ( Fig. 12-2, A ) and protrusion ( Fig. 12-2, B ) of the teeth, both of which result from discrepancies between the size of the teeth and the size of the bony bases. Howe et al. have shown that dental crowding appears to be related more to a deficiency in arch perimeter than to teeth that are too large. A primary factor in dental crowding often is maxillary transverse and/or sagittal deficiency. If the position of the maxillary dentition reflects the skeletal discrepancy, crossbite results; on the other hand, if maxillary constriction is camouflaged by the dentition, and both dental arches are constricted, crowding in the absence of crossbite is observed.
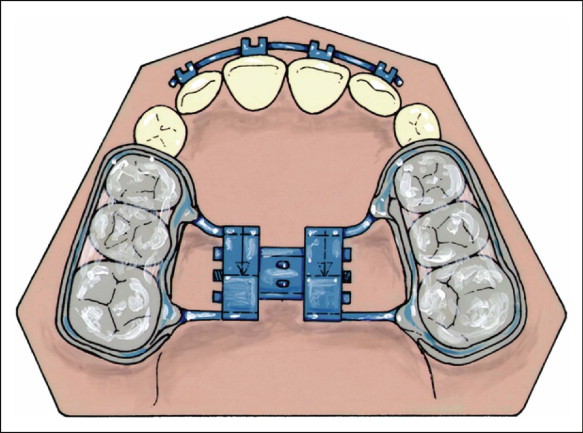
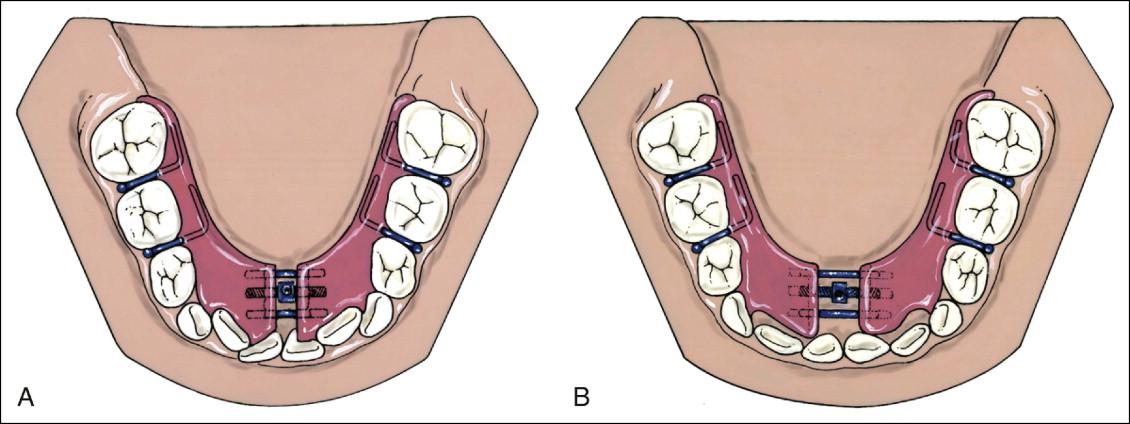
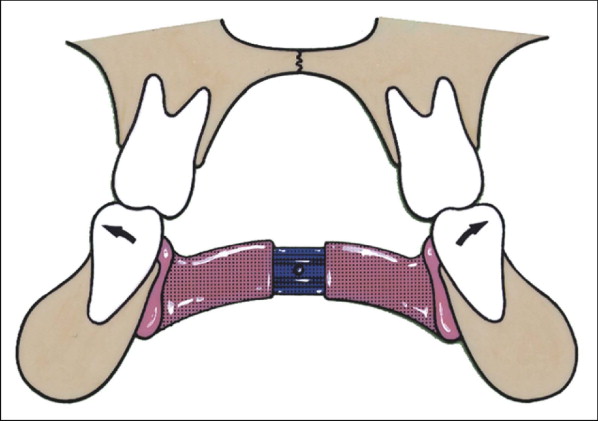
It is well recognized that one of the limiting factors in the management of tooth-size/arch-size problems is available space in the mandibular dental arch. Unfortunately, true orthopedic expansion of the lower arch is not possible, unless recently developed distraction osteogenesis techniques are used. Interestingly, it has been the author’s observation that the position of the mandibular dentition may be influenced more by maxillary skeletal morphology than by the size and shape of the mandible. For example, after RME in the mixed dentition, there is not only expansion of the maxillary dental arch with the acrylic splint expander ( Fig. 12-3 ), but also subsequent spontaneous widening of the lower dental arch in some patients after expansion. In other patients with constricted mandibular dentitions and crowding of the lower incisors, the author often uses a removable lower Schwarz expansion appliance ( Fig. 12-4 ) to upright the lower posterior teeth that have erupted into occlusion in a more lingual orientation because of the associated constricted maxilla. Widening the mandibular dental arch orthodontically before expanding the maxilla orthopedically allows for greater widening of the maxilla by “decompensating” the positions of the mandibular teeth ( Figs. 12-5 and 12-6 ).
Other Clinical Signs of Maxillary Deficiency
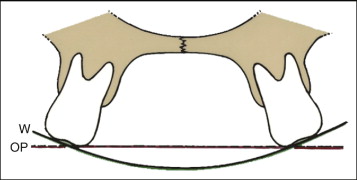
Crossbite and dental crowding are two easily recognizable clinical signs that could be the result of maxillary deficiency. Other effects of maxillary deficiency, however, are not as easily identifiable and often not detected. For example, laterally flared maxillary posterior teeth ( Fig. 12-7 ) may camouflage a maxillary skeletal transverse deficiency. These patients have what appears to be a normal posterior occlusion, although on closer inspection the maxilla is narrow (e.g., intermolar width <31 mm), and the curve of Wilson is accentuated. The lingual cusps of the maxillary posterior teeth extend below the occlusal plane, often leading to balancing interferences during function. Even though there is no crossbite, such patients are candidates for RME before comprehensive edgewise therapy.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


