Maxillary Anterior Direct Build-up with Indices
Subir Banerji and Shamir B. Mehta
Principles
For more challenging anterior tooth wear (TW) cases, there is a need for a protocol that provides the operator with a greater level of control, predictability and contingency planning. This can be accomplished by the use of a diagnostic wax-up, which should be carefully formulated on the basis of an accurate occlusal and aesthetic prescription. The latter may be directly indexed using either a polyvinyl siloxane (PVS) material or a fabricated stone duplicate, which can then be used to form a thermoplastic template to assist with resin composite placement. This chapter will focus on the use of the former.
Cases of anterior TW that may benefit from the use of a more controlled approach include:
- Where there may be extensive TW extending to include a significant portion of the proximal walls
- Occlusal changes that may involve an overall increase in the occlusal vertical dimension, especially where multiple posterior restorations are being planned
- Where attainment of the functional or aesthetic end point may be challenging
- Where is a need to apply resin composite in a ‘layered’ manner.
The five principles for the restoration of worn teeth, as discussed in Chapter 9.3, apply in an analogous manner for all levels of TW, and should be given consideration when planning restorative rehabilitation.
For cases where resin composite is to be used as the dental material of choice, it is important to make sure that a minimum thickness of 1.5–2.0 mm of material is placed in all areas of functional loading. Accordingly, wax patterns should be made to conform to this dimension. The occlusal end point should aim to provide even contacts in the intercuspal position, shared occlusal contacts on mandibular protrusion and a canine-guided occlusal scheme. It should be noted that in cases where there is also TW on the posterior teeth, then this would also need to be addressed. Where it is just localised in the maxillary anterior dentition, the passive axial re-establishment of the posterior teeth following the anterior build-up would allow the desired occlusal contacts to be established and this should be confirmed. There may, however, be a need to include alterations to this generic approach given the individual circumstances, such as the presence of a large direct restoration or endodontically treated tooth (particularly in the presence of a post-retained core).
The aesthetic prescription is perhaps most appropriately established by undertaking an intra-oral mock-up, as described in Chapter 2.5. The use of biometric guides such as those listed in Chapter 9.3 may be helpful.
A number of studies have evaluated the efficacy of resin composite to treat wear of the anterior dentition. A success rate of approximately 90% has been described for labial direct composite veneers reported over a short to medium evaluation period.1–4
Procedures
Carefully inspect the diagnostic wax-up when it is returned from the dental laboratory. Figure 9.4.1 shows the use of a Golden Mean gauge to ascertain the desired proportions. It is worth carrying out an intra-oral mock-up using the information from the wax-up, as described in Chapter 2.5.
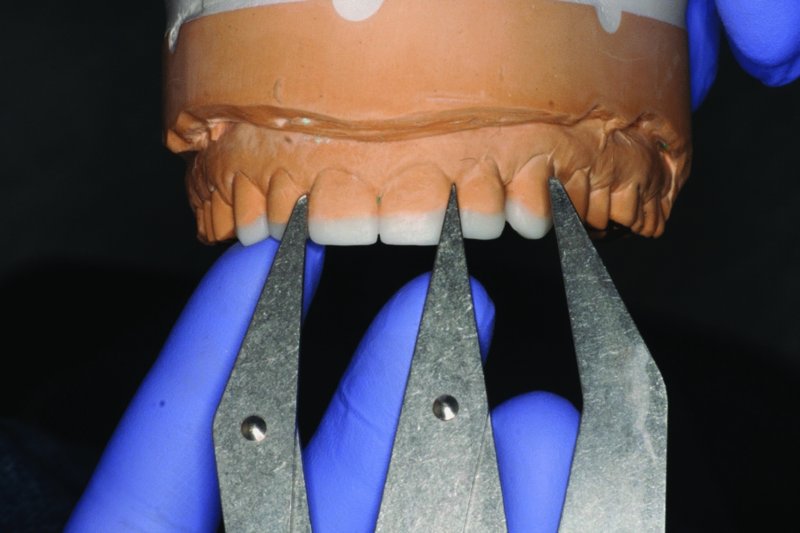
Figure 9.4.1 Verification of a diagnostic wax-up using a Golden Mean gauge
Prepare a palatal silicone index, commonly referred to as a silicone key. An example is shown in Figure 9.4.2. This index will assist you with resin placement in an incremental, layered manner. It will allow the worn-down tooth to be re-constructed in an anatomical way and also optimise resin polymerisation, by applying suitable increment sizes that will permit complete polymerisation. The silicone key will in essence provide a ‘negative’ of the occlusal prescription as established by the wax-up, allowing the occlusal prescription to be ‘copied’.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


