Introduction
Class II subdivision malocclusions with their asymmetric occlusal relationships often pose treatment difficulties. The aim of this study was to evaluate the longitudinal changes of dental arch asymmetry in untreated subjects with Class II subdivision malocclusion.
Methods
From 706 files from the University of Michigan Growth Study, longitudinal records of 17 untreated subjects with Class II subdivision malocclusion were included this study. Dental arch changes at 3 consecutive longitudinal intervals, defined by the cervical vertebral maturation method, were analyzed on digital dental models. The average ages of the subjects were 12.4, 15.1, and 19.1 years at the 3 time periods, respectively. Maxillary and mandibular reference lines were constructed and used for the intra-arch asymmetry measurements. The Friedman test and analysis of variance with repeated measures were used to determine dental arch asymmetries at the P <0.05 level.
Results
All subjects were found to have a type 1 Class II subdivision malocclusion characterized by distal positioning of the mandibular first molar on the Class II side. No statistically significant intra-arch asymmetry changes were found for the maxillary and mandibular dental arches in any time period. Between the baseline and the final follow-up, the data indicated decreases in maxillary and mandibular intercanine arch widths and arch lengths symmetrically.
Conclusions
The results of this study indicate that the dental arch asymmetry in patients with Class II subdivision malocclusions did not improve or worsen with growth.
Angle described Class II subdivision as a separate group of Class II malocclusions characterized by a unilateral Class II molar relationship. Since Class II subdivisions account for up to 50% of all Class II malocclusions and are among the most common dental asymmetries in the orthodontic population, the location and extent of asymmetry are concerns.
The etiology of the asymmetry can be quite complex. It could be dentally related, skeletally related, or a combination of both. Several studies have already reported that the primary factor contributing to a Class II subdivision malocclusion is the distal positioning of the mandibular first molar on the Class II side. A secondary contributor is the mesial positioning of the maxillary first molar on the Class II side. Depending on the origin of the malocclusion, 2 types of Class II subdivision malocclusion can be observed: type 1, characterized by distal positioning of the mandibular first molar on the Class II side, and type 2, characterized by mesial positioning of the maxillary first molar on the Class II side. In type 1 Class II subdivision malocclusions, coincidence of the maxillary dental midline with the facial midline and deviation of the mandibular midline were observed. Type 2 has the opposite characteristics.
Kurt et al evaluated the posterior vertical dimensions of the mandible and concluded that the mandible in Class II subdivision malocclusions does not exhibit unusual skeletal positioning or skeletal asymmetry. Alavi et al concluded that Class II subdivision malocclusions result mainly from unilateral distal positioning of the mandibular first molars irrespective of whether this was due to dentoalveolar or skeletal asymmetry. Rose et al confirmed that Class II subdivision malocclusions occur from distal positioning of the mandibular first molars on the Class II side, but they did not evaluate the anteroposterior positioning of the maxillary first molar as a possible contributing factor to the malocclusion. Azevedo et al evaluated Class II subdivision patients with apparent facial asymmetry and reported that the main component of Class II subdivision is dentoalveolar—primarily distal positioning of the mandibular first molar on the Class II side, and secondarily mesial positioning of the maxillary first molar on the same side. Similarly, Janson et al concluded that Class II subdivision malocclusion was mainly dentoalveolar, and the primary contributor was the distal positioning of the mandibular first molars on the Class II side without unusual skeletal or positional asymmetries. Recently, Minich et al evaluated whether Angle Class II subdivision malocclusions have skeletal or dental asymmetries between the Class II and Class I sides using cone-beam computed tomography. They concluded that there were significant skeletal and dental differences between the Class I and Class II sides, and the dental asymmetries accounted for about two thirds of the total asymmetry.
Based on the principle that occlusal changes can occur in growing and nongrowing subjects with normal occlusion, and because no studies have been published concerning dental arch asymmetry changes in patients with Class II subdivision malocclusion, we conducted this study to evaluate longitudinal growth changes in dental arch asymmetry and to contribute to the knowledge of dental arch changes over time.
Material and methods
The sample was selected retrospectively from the files of the University of Michigan Growth Study; 706 study casts were evaluated for longitudinal records of orthodontically untreated subjects with Class II subdivision malocclusion.
Sample selection was based exclusively on the initial anteroposterior dental relationship, regardless of any other dentoalveolar or skeletal characteristic. The selection criteria were the following.
- 1.
A Class II molar relationship of half a premolar in width or greater on 1 side and a Class I molar relationship on the other side from the buccal aspect, with the mesiopalatal cusp of the maxillary first molar occluding with the mesial triangular fossa of the mandibular first molar from the lingual aspect.
- 2.
All permanent teeth present up to the first molars.
- 3.
No supernumerary or congenitally missing teeth, excluding third molars, or teeth with extensive restorations or gross decay.
- 4.
No ectopic teeth or anomalies in tooth shape.
- 5.
No previous orthodontic treatment.
- 6.
No crowding or, at most, symmetrical crowding up to 3 mm.
- 7.
No anterior or posterior crossbite.
- 8.
Clear lateral cephalograms at 3 time points available for all selected subjects. Additionally, casts with fractured cusps or severe attrition, or with molars or premolars on which more than two-thirds of the occlusal surface had been reconstructed, were excluded.
A final sample size of 17 pairs of dental casts (8 boys, 9 girls) and a total of 68 sides (maxillary and mandibular, right and left) were included for analysis. All subjects were of European-American ancestry. The assessment of the stages of cervical vertebral maturation on the lateral cephalograms for each subject was performed by 1 investigator (B.Y.). The baseline assessment corresponded to stage 3, the second assessment corresponded to stage 4, and the final follow-up corresponded to stage 5. The mean ages at 3 times were 12.4 (±0.1), 15.1 (±0.6), and 19.1 (±0.6) years, respectively.
All plaster models were transformed into digital format by a 3-dimensional (3D) model laser scanner (D250 3D Dental Scanner; 3Shape A/S, Copenhagen, Denmark). The digital models were analyzed by 1 investigator (B.Y.) using the 3Shape Orthoanalyzer software (version 1.0; 3Shape A/S). Cast measurements were based on those of Alavi et al and Sinclair and Little.
On the maxillary digital model, 2 points—the first at the distal aspect of the incisive papilla and the second adjacent to the second rugae—defined the median raphe that was used as the dental midline. Unlike the study by Alavi et al, the posterior border of the raphe near the fovea centralis was not preferred because of poor determination in the digital models. An anterior reference line was constructed perpendicular to the median raphe through the midpoint between the central incisors using the horizontal default position of the software with grids.
The median raphe was transferred to the mandibular model as follows. The top view in the inspection section of the program was selected, the maxillary model was hidden, and the mandible was then visible. Plane offset was adjusted to +50 mm. During this adjustment, the horizontal default position with grids was kept stable. Hence, the median raphe was transferred to the mandible. The anterior reference line was constructed perpendicular to the transferred median raphe through the midpoint between the central incisors using the horizontal default position of the software with grids as well.
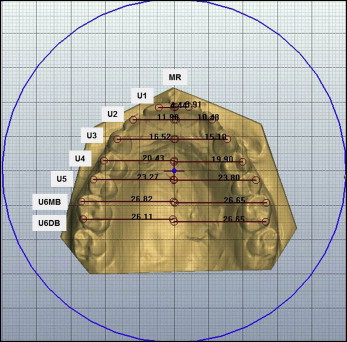
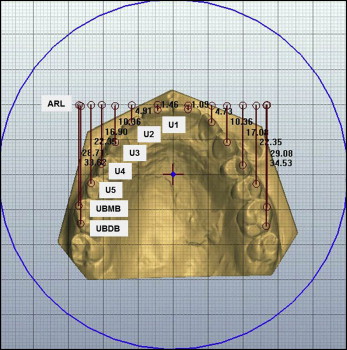
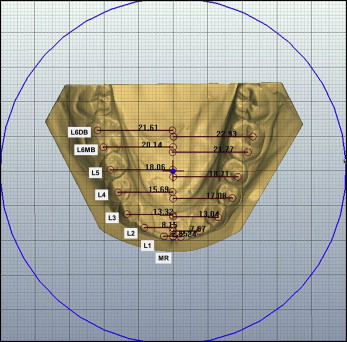
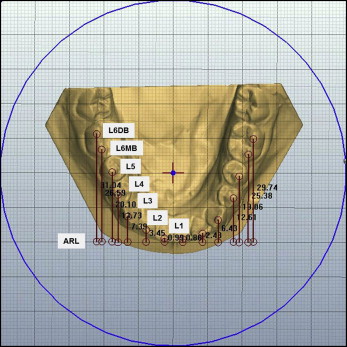
Horizontal measurements were made at 90° to the median raphe from the buccal cusp tips of the posterior teeth, the cusp tips of the canines, and the midincisal edges of the anterior teeth bilaterally; vertical measurements were made at 90° to the anterior reference line from the same tooth landmarks. The linear measurements made from bilateral the tooth landmarks ( Table I ) to the horizontal and vertical reference lines on the maxillary and mandibular dental models are shown in Figures 1 through 4 .
| Abbreviation | Definition |
|---|---|
| U1/L1 | Midincisal edge of upper/lower central incisors |
| U2/L2 | Midincisal edge of upper/lower lateral incisors |
| U3/L3 | Upper/lower canine cusp tip |
| U4/L4 | Upper/lower first premolar buccal cusp tip |
| U5/L5 | Upper/lower second premolar buccal cusp tip |
| U6MB/L6MB | Upper/lower first molar mesiobuccal cusp tip |
| U6DB/L6DB | Upper/lower first molar distobuccal cusp tip |
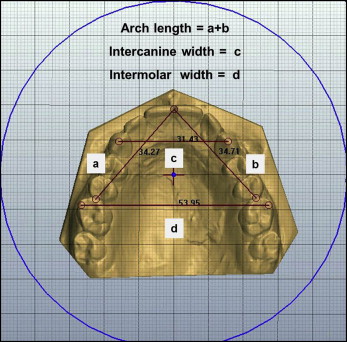
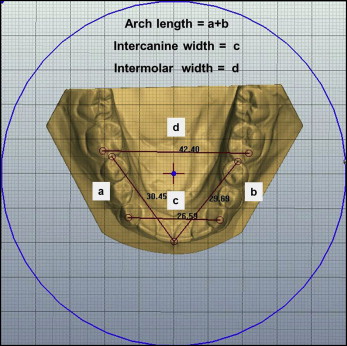
Additionally, intercanine width (distance between cusp tips or estimated cusp tips in cases of wear facets), intermolar width (distance between mesiobuccal cusp tips or estimated cusp tips in cases of wear facets), and arch length (sum of the right and left distances from mesial anatomic contact points of the permanent first molars to the contact points of the central incisors) were measured ( Figs 5 and 6 ).
Asymmetries were calculated by determining the absolute difference between homologous measurements as related to the reference lines. The same procedure was followed to compute the anterior and buccal segment anteroposterior asymmetries. Dental midlines were evaluated by posteroanterior radiographs. On these, a reference midline was determined geometrically so that it passed through the root of crista galli perpendicular to a line connecting the most superior points on the orbital contours.
Ten randomly selected sets of digital models were redigitized and remeasured 2 weeks after the first set of recordings to calculate the method error by the same investigator (B.Y.). The casual error was calculated according to Dahlberg’s formula. The systematic error was calculated with paired-samples t tests at P <0.05. The mean differences of each variable between the successive tracings were compared with the paired t tests. No significant differences were found between the 2 sets of measurements.
Statistical analysis
All data analyses were carried out using SigmaStat (version 3.5; Systat Software, San Jose, Calif). Descriptive statistics, including means and standard deviations, were calculated for between-stage changes. Normal distribution of the data was verified with the Kolmogorov-Smirnov test. Data without normal distribution were compared with nonparametric statistics with the Friedman test, and analysis of variance with repeated measures was used for normally distributed data. All values were considered significant at P <0.05.
Results
Means and standard deviations for all data are listed in Tables II and III . All subjects were found to have a type 1 Class II subdivision malocclusion characterized by distal positioning of the mandibular first molar on the Class II side. No statistically significant intra-arch asymmetry changes were found for the maxillary and mandibular dental arches in any time period.
| Measurement (mm) | Baseline | Assessment 2 | Final follow-up | P | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Upper | |||||||
| U1 to MR | 0.208 | 0.754 | 0.228 | 0.920 | 0.194 | 1.463 | 0.790 |
| U2 to MR | 0.005 | 0.769 | 0.005 | 0.858 | 0.310 | 2.370 | 1.000 |
| U3 to MR | 0.088 | 1.253 | 0.119 | 1.137 | 0.311 | 1.317 | 0.954 |
| U4 to MR | 0.062 | 0.940 | 0.255 | 0.985 | 0.509 | 1.475 | 0.589 |
| U5 to MR | 0.578 | 1.169 | 0.196 | 1.243 | 0.000 | 1.621 | 0.289 |
| U6MB to MR | 0.584 | 1.184 | 0.258 | 1.669 | 0.093 | 1.409 | 0.338 |
| U6DB to MR | 0.639 | 1.408 | 0.026 | 1.678 | 0.174 | 1.514 | 0.327 |
| Intercanine width | 34.265 | 1.564 | 34.274 | 2.164 | 34.086 | 2.021 | 0.707 |
| Intermolar width | 51.495 | 1.529 | 50.112 | 6.482 | 51.538 | 1.677 | 0.838 |
| Arch length | 70.356 | 3.439 | 69.373 | 2.826 | 68.915 | 2.782 | 0.080 |
| Lower | |||||||
| L1 to MR | 0.225 | 2.823 | 0.054 | 2.715 | 0.114 | 2.911 | 0.790 |
| L2 to MR | 0.060 | 2.408 | 0.709 | 3.030 | 0.343 | 3.117 | 0.205 |
| L3 to MR | 0.144 | 2.242 | 0.574 | 2.658 | 0.388 | 2.420 | 0.662 |
| L4 to MR | 0.194 | 1.744 | 0.047 | 1.991 | 0.126 | 1.968 | 0.790 |
| L5 to MR | 0.051 | 1.383 | 0.098 | 1.877 | 0.599 | 2.242 | 0.322 |
| L6MB to MR | 0.494 | 1.305 | 0.064 | 1.986 | 0.452 | 2.278 | 0.197 |
| L6DB to MR | 0.603 | 1.456 | 0.230 | 1.844 | 0.080 | 1.938 | 0.443 |
| Intercanine width | 26.259 | 1.286 | 25.976 | 1.719 | 25.664 | 1.299 | 0.080 |
| Intermolar width | 44.486 | 2.041 | 44.251 | 2.210 | 44.095 | 2.119 | 0.217 |
| Arch length | 60.846 | 2.504 | 59.546 | 2.347 | 58.931 | 2.372 | <0.001 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


