Fig. 8.1
Lower-lip pits in a child with a bilateral cleft lip and palate. (a) Before lip surgery. (b) After lip surgery at 6 months
Fig. 8.2
(a) Pits in the upper and lower lips in a 20-year-old with a bilateral cleft lip and palate. (b) Close-up view

Fig. 8.3
Lip pits in the upper and lower lips in a bilateral cleft lip and palate

Fig. 8.4
Radiograph of a premaxilla showing two central and one lateral incisors (left) and twined lateral incisors and one malformed central incisor (right)

Fig. 8.5
Missing and malformed anterior teeth. (a) A very small premaxilla with one deciduous incisor but no permanent tooth buds. (b) Malformed deciduous maxillary anterior teeth and missing left deciduous anterior teeth
8.1.2 Frequency
No survey of lip pits has been carried out among the general population; hence, the frequency of this rare anomaly has been only roughly estimated from its incidence in hospital records.
Assuming that 70 (Gorlin and Pindborg 1964) to 80 % (Van der Woude 1954) of patients with pits of the lower lip have associated cleft lip and/or palate and that the frequency of clefts is 1:650 (one in every 650 births), it can be estimated that the frequency of lip pits among the general population is about 1:75,000–1:100,000 (one in every 75,000–100,000 births).
8.1.3 Morphology
Fistulas of the lower lip usually appear as two pits or humps on the vermilion portion of the lower lip, generally equidistant from the midline. Various kinds of asymmetry may be observed with regard to the midline, or one pit may be positioned more orally. Some pits are mere depressions; others are channels 10–15 mm deep with openings at the top of nipple-like elevations. Some secrete small amounts of viscous saliva but most are asymptomatic.
In exceptional cases, only one pit is present, which may be located either centrally or on one side or the other of the midline of the lower lip. Some cases of single lip pit have occurred in families with members with double lower-lip pits. It can be assumed that a single pit is not a distinct entity but rather an incomplete expression of the trait. On the other hand, the rarely described fistulas of the upper lip (Lannelongue 1879; Radcliff 1940) have not shown any inheritance pattern.
Commissural or angular lip pits – small, usually asymmetrical channels located at the lip angles – are also distinct entities with a much higher incidence and different embryology (Gorlin and Pindborg 1964; Lemke 1959; Everett and Wescott 1961; Witkop 1964; Witkop and Barros 1963; Schuermann et al. 1966).
8.1.4 Association with Other Malformations
In addition to their strikingly common association with cleft lip and/or palate, pits of the lower lip have been noted in association with other malformations. Gorlin and Pindborg (1964) have found cases of lip pits along with anomalies of extremities, popliteal pterygia, and anomalies of the genitourinary system. The association with cleft lip and/or palate may well form a distinct new syndrome.
A review of the literature suggests that a variety of other anomalies may be associated with lip pits. Among them: syndactyly of the hands together with cleft lip and palate (Lannelongue 1879; Bernauds 1906); mental retardation and cleft, type not specified (Test and Falls 1947); ankyloglossia and cleft lip and palate (Van der Woude 1954); polythelia (Baxter 1939); symblepharon and cleft lip and palate (Oberst 1910); and ankyloblepharon, adhesion between the maxilla and mandible, and cleft uvula (Neuman and Shulman 1961). In two cases of the orofacial digital syndrome, pits were observed by Gorlin and Psaume (1962).
8.1.5 Inheritance
In most cases of lip pits described during the last 120 years, a marked hereditary pattern was observed. Although all authors have excluded autosomal recessive inheritance or X-linked inheritance, there is no uniform opinion concerning whether or not the condition is due to a single autosomal dominant pleiotropic gene.
Fogh-Andersen (1942, 1961) was the first to clearly point out that the inheritance of clefts in the families with a history of lip pits is of a different character than in families where no lip pits occur. According to Fogh-Andersen (1942, 1961), the role of genetic factors in families with lip pits is much more pronounced, and both genetically different types of clefts (cleft lip or cleft lip and palate and isolated cleft palates) commonly are found within a single family. Fogh-Andersen also stated that in families in which fistulae of lower lip occur as a dominant hereditary character, there are some cases of cleft lip and cleft palate alone. Possibly, it may be explained as the result of coupling of neighboring genes.
Van der Woude (1954), in a careful study of five pedigrees with clefts and lip pits, found that the combination of pits and clefts is based on a single dominant gene of variable expressivity. She agreed with other authors (Test and Falls 1947) that a mildly affected individual can pass the trait on in a very severe form and a severely affected individual can pass the trait on in mild form. The sex of the individual is not a factor in passing on this anomaly. No sex limitation or preference exists.
Patients with clefts but without lip pits (or their parents) often ask for genetic advice. In most of these cases, only a small risk of cleft lip (less than 10 %) is indicated for the next child. But the counseling situation is significantly changed when associated lip pits are found. In this instance, all clefts in the family are considered part of the syndrome, and risk figures for clefts are remarkably higher.
8.1.6 Evidence of Heterogeneity
It is also clear that the risk of a cleft occurring in a child is significantly higher when the parent has lip pits and a cleft than when the parent has lip pits only. Two alternative explanations for this heterogeneity between families can be considered: (1) The development of clefts in persons carrying a “lip pit” major gene may be influenced by modifying genes at other loci, and (2) in some families, a mutant allele may produce lip pits with only occasional clefts, whereas in other families a different mutant allele (at the same or a different locus) may frequently lead to clefts in addition to lip pits. Thus far, efforts to use the data to support one or the other of these hypotheses have been unsuccessful. Cervenka et al. (1967) reported data from 66 individuals with lip pits in his study and 446 cases with lip pits from the literature with known sex to establishing a 1:1 sex ratio. The frequency of the syndrome was estimated as 1:75,000–1:100,000 in the white population.
Cervenka et al. (1967) further states that family histories can be explained adequately on the basis of autosomal dominant inheritance with variable expressivity of the trait. Penetrance is high, estimated at 80 %. Pits show up more frequently than clefts, and there is a significant association between the types of clefts in parents and their children. Possibly, the development of clefts in this syndrome is influenced by modifying genes or by different mutant alleles with a predilection for the different types of cleft.
8.2 Orthodontic Treatment, Dentition, and Occlusion
8.2.1 Crossbite Correction (Figs. 8.6, 8.7, 8.8, 8.9, 8.10, 8.11, and 8.12)
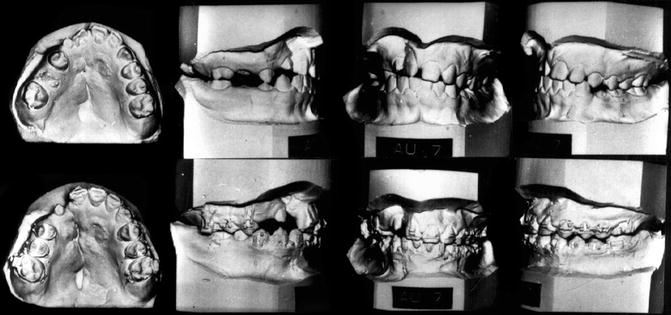
Fig. 8.6
Palatal expansion increases nasal width. At 12 years of age, buccal crossbite correction of the cleft segment was performed by palatal expansion. Crossbite correction is orthopedic in that the cleft bony segment is moved laterally, widening the nasal chamber on that side. Top: Right buccal segment is in crossbite. Bottom: After expansion: Palatal fistulae are exposed with the separation of the overlapped palatal segments
Fig. 8.7
(a) Fixed palatal helix expander used in deciduous dentition with or without an anterior finger spring. (b) Fixed “Arnold” expander using a compressed open coil spring to create an expansion force
Fig. 8.8
(a–c) Crossbite correction for bilateral cleft lip. (a) Age 2 years 8 months. Note the bilateral crossbite. (b) Arnold expander in place. (c) Crossbite correction after 3 months brought on by the outward movement of the lateral palatal segments
Fig. 8.9
(a–h) Correction of anterior and posterior crossbite in the deciduous and mixed dentition in a severely scarred palate. (a) Complete unilateral cleft lip and palate, unoperated. (b) Palatal segments in contact. (c) Palatal cleft closed at 6 months of age: von Langenbeck procedure was used to close a very wide cleft space. (d) Bilateral buccal and anterior crossbite. (e) Arnold expander is in place. (f) Crossbite is still present due to excessive scar tissue. (g) Expander is fully extended in the early mixed dentition. (h) Anterior crossbite was corrected, but the buccal crossbite is still present. Comments: The severely scarred palate prevents the lateral movement of the medially positioned palatal segments. Scars can only be stretched a slight amount, and if that amount is exceeded, the bony segments will not move, and instead the teeth will respond to the orthodontic forces. Should the teeth be tipped outwardly they will have to be permanently retained by a bridge or by teeth splinting
Fig. 8.10
(a, b) Anterior and buccal crossbite correction the mixed dentition. (a) Anterior crossbite was due to palatally displaced deciduous teeth with premaxillary segment and not to growth deficiency. The buccal teeth are in crossbite as a result of the lesser palated segment being palatally displaced. This picture has the maxillary anterior teeth in crossbite; the lower anterior teeth are shown while the upper teeth are hidden. (b) A fixed palatal expander with finger springs is used to expand the arch and advance the anterior teeth. In most instances, it is unnecessary to disocclude the anterior teeth to move them forward. Buccal expansion depends on the ability of the lesser bony segment to move outward. Retention of the bony correction is essential
Fig. 8.11
(a) Orthodontic correction of an anterior and posterior crossbite in the permanent dentition. Anterior dental crossbite does not necessarily mean that the maxilla is anteroposteriorly deficient in size and requires a LeFort I advancement. In this case, the maxillary dentition was advanced orthodontically with the missing lateral incisor space opened to achieve interarch congruency. The expansion was maintained by complete arch splinting. (b) A severely ventroflexed premaxilla was uprighted during the deciduous dentition. In order to maintain the correction after the deciduous anterior teeth are lost, a fixed palatal retainer with an acrylic button is placed on the premaxilla’s palatal incline
Fig. 8.12
(a, b) Repaired bilateral cleft lip and palate. An anterior openbite and retruded premaxilla resulting from inadequate orthodontic and surgical planning. (a) A slight anterior openbite was present at 8 years of age at which time a secondary alveolar bone graft was performed. The orthodontist attempted to close the lateral incisor spaces by bringing the cuspids mesially, while retracting the central incisors. This created a more severe openbite and an anterior crossbite. (b) The orthodontic mechanics were reversed. The lateral incisor spaces were opened, and the central incisors were advanced into an ideal overbite and overjet relationship. One of the bone grafts had to be redone. Comments: When the buccal occlusion is Class I, it is always better to keep the lateral incisor space open in both bilateral and unilateral cleft cases. There are occasions when a mandibular central incisor will need to be extracted in order to avoid flaring the maxillary central incisors and to obtain a proper occlusion. An anterior fixed bridge will stabilize the arch and replace the missing maxillary lateral incisors
Bergland and Sidhu (1974) advocated postponing orthodontic treatment until complete eruption of the permanent anterior teeth. Segmental alignment can then be corrected with simultaneous manipulation of the anterior teeth. We believe it is best to start maxillary arch expansion when the deciduous dentition is completely erupted and when the children can be easily managed. A three-phase treatment is followed: (1) Buccal crossbite is corrected at 4–6 years, (2) anterior teeth are aligned at 8–9 years, and (3) final orthodontics is utilized at 11-plus years.
Crossbite correction by moving palatal segments laterally in the presence of extensive palatal scarring is difficult and often unsuccessful. Extensive mucoperiosteal undermining, leaving wide denuded palatal bone, was necessary to close the wide palatal cleft at 6 months of age. Uniting the lip moved the palatal segments together (molding action) into good arch approximation. Palatal scar contracture moved the buccal segments farther medially, placing the buccal teeth in crossbite. The anterior dental crossbite does not necessarily reflect diminished anteroposterior maxillary growth but, rather, malposition of the premaxillary teeth of the greater segment.
8.2.1.1 Unilateral Cleft Lip and Palate
Deciduous and Mixed Dentition: When the smaller segment’s alveolar process is contained within the premaxillary alveolar segment of the larger segment, a dental crossbite occurs between the maxillary and mandibular teeth. Dental dysplasia (eruption of a tooth out of position) may or may not coexist with segmental dislocation. A simple crossbite of one tooth may be due to its malposition rather than to the palatal segment’s collapse. The most frequent crossbite is brought on by the mesioangular rotation of the lesser segment rather than by ectopic tooth eruption. Total buccal crossbite is seen less frequently but is generally present when the palatal tissue is scarred. In either case, the same helix type of palatal expander can be utilized and correction achieved within 2–4 months. Anterior movement of the deciduous central incisors often requires lingual undercuts either by orthodontic bands with lugs or by direct lingual shelf bonding to stabilize the anterior activated palatal finger springs.
A fixed palatal retainer can hold the correction until the second stage of orthodontic therapy is initiated. There is no way to predict the return of a crossbite in the absence of permanent retention. Bone grafting across the alveolar cleft does not guarantee retention of the corrected arch form.
Permanent Dentition: In Class I and Class III cases, it is usually preferable to open the missing lateral incisor space with the expectation of utilizing a fixed bridge to stabilize the corrected arch form and replace the missing tooth. In Class II cases, it may be possible to encourage the cuspid to erupt through the alveolar bone graft in the lateral incisor space, which eliminates the need for extensive orthodontics and bridgework. The cuspid may need to be splinted to the central incisor in order to maintain the corrected arch form.
8.2.1.2 Bilateral Cleft Lip and Palate
First Stage: Between the ages of 4 and 6 years, the premaxilla is usually ventroflexed and overlaps one or both lateral palatal segments, which may be in partial or complete buccal crossbite. As in unilateral cases, treatment of bilateral cleft lip/palate necessitates moving bony segments into the surrounding muscle ring. If the premaxilla is to be moved forward, bands with lingual lugs are placed on the deciduous central incisors. A fixed helix-type palatal expander with anterior activated finger springs is cemented to the second deciduous molars. The finger springs are positioned under the central incisor-banded lugs for retention. The premaxilla is uprighted prior to correcting the buccal crossbite. The anterior and buccal crossbite correction can be completed within 6 months. As the premaxilla and lateral palatal segments are moved outward, the anterior cleft space is uncovered. A fixed palatal retainer with an acrylic anterior extension to cover the anterior cleft space is placed and kept in position until the alveolar cleft is bone-grafted and all fistulas are surgically closed. Permanent complete palatal retention is necessary, even after alveolar bone grafting. A premaxillary retainer must be placed when the deciduous anterior teeth are lost.
Second Stage: At 7–8 years of age, when the deciduous incisor teeth are replaced by permanent incisors, the anterior crossbite may have to be retreated. The incisors may be rotated and malpositioned. Orthodontic brackets are placed in the upper arch to support a labile arch wire, which will be utilized to reposition the incisor teeth and reduce the premaxillary overbite. A pontic tooth with band is placed on the arch wire to achieve a more pleasing aesthetic result. The premaxilla needs to be properly aligned with the lateral palatal segments prior to alveolar bone grafting; this procedure may be performed between 7 and 9 years of age. A lateral incisor as well as a cuspid may erupt through the area of new bone formation.
Third Stage: Children at 10+ years of age are treated as any other child. The many malocclusion possibilities render it impossible to develop treatment plans for each contingency; instead, basic treatment problems are discussed:
1.
Class I malocclusion (with anterior and/or buccal crossbite): The crossbite generally is due to lingual bony displacement. The upper arch should be advanced and expanded. If there is sufficient arch length, the missing lateral incisor area is left open. In arch shortage cases, it may be preferable to move the cuspid adjoining the space into the lateral incisor area rather than extract the first bicuspid on that side. A number of variations of treatment exist according to tooth size and location.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


