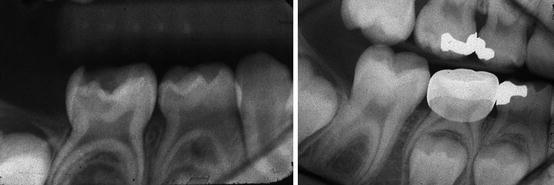
Fig. 4.1
An open lesion in the distal of the second primary molar is slower growing and dark in color. The first permanent molar has a closed lesion which progresses faster, is moist, and has a yellowish color inside (Photograph courtesy of Dr. N Sue Seale)
The closed lesion has a homogeneous mixture of lactobacillus subspecies and progresses faster while the open lesion has many different bacterial species and is slower growing [10]. The clinical implication from cariology for a closed lesion is that caries progress is accelerated and may not allow reparative dentin formation to prevent the caries reaching the pulp quickly. Proper caries excavation, without removing the entire lesion, can avoid a pulp exposure. An open lesion progresses slower, usually allowing reparative dentin formation that can prevent pulp exposures [7].
4.4 Methods of Caries Excavation
4.4.1 Complete Excavation
Traditional operative dentistry approach to deep caries treatment advocated its total removal using slow-speed rotary burs and hand instruments [11]. Complete excavation removes all the infected and affected dentin.
4.4.1.1 Complete Excavation and Rate of Pulp Exposure
A pulp exposure can occur when complete excavation of deep caries is employed. A meta-analysis revealed that complete caries excavation of deep caries in primary and permanent teeth has three times the odds ratio of creating a pulp exposure compared to partial excavation [12]. Another systematic review of pulp exposures after complete excavation demonstrated that partial caries removal reduced the incidence of an exposure by 77 % compared to complete excavation [13].
In 1990, Elderton [14] claimed that most restorations were replacement restorations due to caries and/or restoration failure. This replacement of restorations could result in a very thin amount of dentin covering the pulp. The amount of remaining dentin under a restoration has been shown to be the most critical factor in determining the future health of the pulp [15] (see Chap. 2). In a closed carious lesion with extensive moist dentin, complete excavation will greatly thin out the remaining dentin. Therefore, over-excavation is not recommended [7].
4.4.1.2 Complete Excavation and Direct Pulp Capping for Primary Teeth
Performing direct pulp capping after complete excavation of deep caries is contraindicated in primary teeth due to the unreliable outcomes [16]. In addition, as described in Chap. 5, pulpotomy would likely be indicated and have a higher success rate. For a traumatic exposure or a mechanical exposure occurring during cavity preparation of shallow decay, performing a direct pulp capping with calcium hydroxide or mineral trioxide aggregate (MTA) is indicated [1].
4.4.1.3 Complete Excavation and Direct Pulp Capping for Permanent Teeth
Direct pulp capping after pulp exposures resulting from excavating deep caries has been shown to have low success in permanent teeth [17, 18]. In a randomized multicenter study on direct pulp capping or partial pulpotomy with calcium hydroxide involving 58 patients with exposed pulps after caries excavation in permanent teeth, the authors reported a low success rate (31.8 % vs. 34.5 %, respectively) and no significant difference in pulp vitality between the two pulp capping procedures after a 1-year or more follow-up [17]. Al-Hiyasat et al. [18] found that carious exposures had a 33 % pulp capping success compared to 92.2 % success for a mechanical exposure.
Another method for treating a pulp exposure after complete excavation in permanent teeth was described by Bogen et al. and had a much higher success [19]. In this retrospective report, the author recommended creating, on purpose, a large pulp exposure, rinsing extensively with sodium hypochlorite to control the bleeding, placing MTA on the pulp followed by a temporary filling. A second visit was required to place a final restoration. This procedure resulted in a 98 % success in 49 teeth after almost 4 years.
4.4.2 Stepwise Caries Excavation (SW)
The second method of deep caries excavation is termed stepwise excavation and is done over two patient visits. The first excavation is intended to remove the superficial necrotic, infected, and affected dentin by completely excavating the periphery of the lesion. This excavation does not excavate caries near the pulp to avoid a pulp exposure [20]. A retentive temporary restoration is placed leaving soft, moist, discolored dentin on the pulpal floor. The dentin is then covered with calcium hydroxide and a self-setting glass ionomer temporary filling [17] (Fig. 4.2). A resin-modified glass ionomer has also been advocated in place of the self-setting glass ionomer [21]. SW is intended to allow remineralization of the affected dentin and formation of more tertiary dentin [20]. The carious lesion is reentered in 8–12 weeks by removing the temporary, and a final complete excavation is done leaving only central yellowish or grayish hard dentin in the pulpal floor (Fig. 4.3). A final restoration is placed with the intention to seal the pulp from any microleakage [17]. In two systematic reviews and meta-analysis studies [12, 13], SW significantly reduced pulp exposures compared to complete excavation (Fig. 4.4).

Fig. 4.2
Mandibular right first permanent molar presented with a history of pain when chewing foods of short duration (initial radiograph). No other signs or symptoms in this 12-year-old patient (left). Periapical film shows posttreatment first visit stepwise excavation with a calcium hydroxide base and a reinforced zinc oxide temporary filling in place (right)
Fig. 4.3
Same mandibular first molar 8 weeks after the second stepwise excavation showing the hard dark dentin on the pulpal floor and the complete peripheral excavation (left). The right photograph shows a resin-modified glass ionomer base prior to steel crown placement
Fig. 4.4
Same mandibular permanent molar 48 months after stepwise excavation and indirect pulp treatment. The tooth was asymptomatic and the radiograph showed no pathology
4.4.3 Partial (Incomplete) Caries Excavation
The third type of caries excavation is termed partial or incomplete excavation involving one appointment removal of the peripheral decay but intentionally leaving the deepest caries in place to avoid a pulp exposure. An indirect pulp treatment is then completed (Fig. 4.5).
Fig. 4.5
Preoperative view (left) and radiograph (center) of a mandibular left second primary molar with deep dentinal caries. View of the partial excavation showing peripheral caries removed but the deeper caries is left in place (right). An indirect pulp treatment was then performed
Partial excavation omits the reentry and second excavation done in SW by sealing off the caries with a final restoration placed at the same appointment [12] (Fig. 4.6).

Fig. 4.6
Same second primary molar as Fig. 4.5 treated in one appointment showing a resin-modified glass ionomer base used as the IPT medicament (left) and then cementation of the steel crown with glass ionomer cement (center). The radiograph (right) shows the tooth 18 months later without history of pain, normal soft tissue, and no pathology
Partial excavation attempts to shift the microbial balance within the affected dentin to promote dentin remineralization and arrest the carious lesion [22]. Maltz et al. [23, 24] published the results of one randomized controlled trial (RCT) comparing stepwise to partial excavation in 299 permanent molars in two time frames. The results of the 2- and 3-year follow-up showed significantly higher success rates of one appointment partial caries excavation compared with SW (96 % and 91 % compared with 81 % and 61 % after 2 years and 3 years, respectively). Maltz et al. speculated on why stepwise excavation success was only 61 % after 3 years [24]. The authors felt some SW patients did not return for the final excavation and restoration in 1–2 months, and the success rate in these patients was very low (13 %). Patients treated with SW that had a final excavation and permanent restoration had survival rates not statistically different from those of partial excavation (88 % with SW vs. 91 % partial excavation) [24].
4.4.4 No Caries Excavation
The last form of caries treatment has been reported in primary teeth. It involves no drilling or excavation of any caries and would be termed no caries excavation. A steel crown to seal the caries and stop its progress is used [25]. The technique is termed the Hall technique (named after Norma Hall, a Scottish dentist) and presumes that sealing the infected and affected dentin from microleakage will arrest the caries [25, 26]. There have been published reports testing the Hall technique success versus conventional restorations [27, 28]. Ludwig et al. [27] reported in a retrospective study that 65 of 67 steel crowns placed using the Hall technique were successful after a meantime of 15 months. In an RCT report after 12 months, the Hall technique crowns were significantly better (p = 0.002) than using conventional complete excavation and a compomer restoration [28]. Whether the Hall technique is indicated for use in teeth with deep dentinal caries is yet unknown. In a 10-year prospective study [29], frank carious lesions in permanent teeth that extended radiographically into less than half the dentin were sealed. No caries excavation was done, and the caries was sealed in place with a self-setting occlusal sealant. The report showed arrest of the lesions over 10 years if the occlusal sealant stayed intact. The study’s purpose was not intended to promote leaving caries unexcavated, but to show if caries was sealed in place by a sealant, it would not progress [29].
4.5 Indirect Pulp Treatment (IPT)
IPT is a vital pulp treatment where the deepest caries is left unexcavated to avoid causing a pulp exposure due to caries excavation. IPT is indicated for primary and permanent teeth [1]. IPT involves two major suppositions for its success: correctly diagnosing that the pulp is vital and placing a final restoration that prevents microleakage [1, 30]. Reaching the correct pulpal diagnosis in primary teeth will be discussed in detail in Sect. 4.6. Preventing microleakage can be achieved through the use of immediate steel crown placement or a well-bonded composite restoration [31, 32].
4.5.1 Indirect Pulp Treatment Procedure
The IPT procedure is normally done in one appointment but can be done as a modification of the SW procedure in two visits. An IPT begins with removal of the superficial infected dentin using a high-speed water-cooled bur [33]. First, the decay in the periphery of the lesion is excavated completely using slow-speed burs such as #4 or #6. Using the same slow-speed bur, partial excavation of superficial decay on the pulpal floor is done, leaving some decay and not exposing the pulp [33]. Using an excavator for the pulpal floor, excavation may remove large pieces of dentin, which can result in a pulp exposure. The amount of decay remaining appears not to be critical, as dentin remineralization occurs irrespective of the amount of decay remaining [34, 35]. The decay remaining is mostly affected dentin. It may appear moist and soft or dark and leathery, but the dentin color and consistency are not critical to IPT success. If a biological seal is created with a final restoration, the remaining bacteria in the dentin are believed to be nonviable, and the affected dentin will remineralize and become harder [20, 34]. A steel crown or a well-bonded composite resin will prevent any microleakage and maximize the likelihood of success (Fig. 4.7).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


