18
Growing Patients
After first permanent molars and incisors erupt, clinicians face a mixed dentition period in which they have to determine whether if there is need for an orthopaedic/orthodontic treatment or not, mostly related to skeletal rather than dental correction. Based on this, phase I treatment is usually done early in this period.
To create a treatment plan practitioners must understand the growth and development patterns, as jaw growth affects orthodontic treatment. For this, we have to focus on our knowledge of mixed dentition and growth in order to determine whether if early treatment has a benefit to patients.

Fig. 18.1 Skeletal growth pattern has to be carefully evaluated in growing patients.
Clinicians must therefore diagnose and intercept certain developing problems with early treatment, while in other cases treatment should wait until permanent teeth have fully erupted, depending on clinical and social aspects related to the patient.

Fig. 18.2 Upper temporary spacing is 3 mm, on average, while tooth discrepancy between these and permanent ones is 7.6 mm, therefore giving a tendency to crowding.
To summarize, when crowding is severe intercanine distance has to be accelerated (6–8 years old in boys, 6–9 years old in girls) to prevent permanent severe crowding and increase arch development. Achieving arches with widths of 35–39 mm leads to prevention of extraction, and hence to better dentoskeletal and muscular adaptation.1

Fig. 18.3 Severe crowding on temporary teeth leads to future extractions or more complex treatments, suggesting that it must be addressed at an early stage.
In deciding whether if early treatment is convenient or not, the clinician should focus on growth peaks, following the clinical considerations established by Bacetti et al.2

Fig. 18.4 Disjunction and protraction should be performed on EC1, while mandibular advancement is should be planned on EC3/4.
Disjunction cannot be performed exclusively with aligners, so mixed treatment with functional devices has to be considered, as we will learn later in this chapter. This is mandatory for class III patients, in which anterior crossbite also has to be resolved.

Fig. 18.5 Anterior crossbite management should be addressed early.
The same applies to class II patients if overjet is higher than 6 mm, regardless of whether it has a skeletal or exclusively dental component, as it reduces the risk of trauma on anterior incisors. Thanks to aligner improvements this can be achieved solely with Precision Wings, avoiding uncomfortable old functional devices such as Klammt or Twin Block.

Fig. 18.6 Skeletal class II can be achieved before than usual if overjet is >6 mm.
The advantages of aligners technique in these patients are clear:
- Single device use instead of different classic orthodontic treatments (functional, braces, wires, etc.), which leads to comfort and easy use and comprehension
- Enhanced dental hygiene
- Digital control of growth with ClinCheck models and iTero scans
- Easy to replace devices if they are lost or broken
- Compatible with sports or any other activities
For this, we strongly suggest treating growing patients with aligners, which will lead to happier patients and improved treatment outcomes.
It is also important for the orthodontist to understand that simpler devices such as Schwartz expansion devices offer simple solutions to basic problems, but good aligner management leads to good outcomes with wider objectives in the first treatment phase.

Fig. 18.7 More simple devices can achieve less objectives than aligners.
18.1 First Treatment
18.1.1 Upper Maxillary Compression

Fig. 18.8 Upper compression with posterior and anterior crowding.
Diagnosis
An 8‐year‐old patient with normodivergent skeletal class I presented with missing 55 and mesial ectopic eruption of 16. They had maxillary compression, deep bite and upper and lower crowding.
Treatment Plan
- Transversal expansion by Hyrax (Hygienic Rapid Expander) for basal expansion and distalization of 16 to open space for 15
- After 8 months with the Hyrax, the patient did not receive any more treatment until the complete eruption of 11 and 21; by that time the patient was 10 years old
- The case was sent to receive Invisalign FIRST treatment and correct the upper and lower crowding and the posterior deep bite that generated after the upper incisors’ eruption
Requirements for the Technician
- In the maxilla, dentoalveolar expansion was requested to open space for 13 and 23 and to provide space for aligning the upper incisors
- Further distalization for 16 was requested until eruption of 15
- In the mandible, crowding was requested to be solved by expansion and lower proclination
- To solve the deep bite, we asked for intrusion of the lower incisors
- No IPR was requested for the case
Treatment Summary
- Patient wore a Hyrax for 8 months and currently has been using the aligners for 1 year on a 7‐day intervals protocol, after the eruption of 33 and 43 in the middle of the first set of aligners
- Additional aligners were requested to cover the upper and lower canines once they had erupted

Fig. 18.9 Views with the Hyrax before Invisalign First.

Fig. 18.10 Panoramic X‐ray before Hyrax.

Fig. 18.11 After the Hyrax and before Invisalign First (10‐year‐old patient).

Fig. 18.12 Panoramic X‐ray before Invisalign First.

Fig. 18.13 Upper CC superimposition and instructions to CAD designer.

Fig. 18.14 Lower CC superimposition and instructions to CAD designer.

Fig. 18.15 Right ClinCheck view, initial situation.

Fig. 18.16 Left ClinCheck view, initial situation.

Fig. 18.17 Attachments can be seen in several areas of the ClinCheck software.

Fig. 18.18 Pretreatment intraoral views (left, front, right) before Invisalign First.

Fig. 18.19 Intraoral views (left, front, right) with first aligner.

Fig. 18.20 Actual situation in additional aligners.

Fig. 18.21 Initial and final occlusal (upper and lower).

Fig. 18.22 Initial and final smile.
18.1.2 First Severe Crowding Treatment

Fig. 18.23 Severe crowding impeding proper lateral incisor eruption both in upper and lower jaw.
Diagnosis
A 7‐year‐old boy a hypodivergent skeletal class presented with severe crowding, left tipping of lower incisors, blocking 32 eruption, facial competence and gummy smile.
Treatment Plan
- Open space for lower laterals, centring lower midline by lower incisor straightening.
- Open space for upper laterals
- Achieve left molar class I
- Improve overjet
- Centre midlines
- Solve anterior crossbite, as upper lateral incisors erupted during treatment on a palatal position
ClinCheck1: Requirements for the Technician
- Request opening space for laterals centring midline simultaneously to this
- Distalize sequentially second quadrant, and planned without using class II elastics, in order to gain overjet by upper incisor protrusion
Fig. 18.24 Taking advantage of aligner biomechanics by distalizing the second quadrant, which led to anterior protrusion and mesialization.
- Expansion was requested in both upper and lower jaw, to correct posterior compressed torques and create bigger arches
Treatment Summary
- Treatment time was 18 months for the first phase
- Second phase will come with eruption of permanent teeth
- Left molar class I relationship was achieved
- Midlines were centred and direction of permanent tooth eruption improved
- Better eruption guide for 33 owing to lower incisor straightening
- Better position for 24, 25, after distalization of 26
- Improvement of smile
- Space gain for teeth alignment
- Transversal arch development

Fig. 18.25 Pretreatment intraoral views (right, front, left, upper, lower).

Fig. 18.26 Pretreatment panoramic X‐ray showing current dentition status and lack of space for lateral incisors as well as second quadrant teeth.

Fig. 18.27 Initial extraoral views.

Fig. 18.28 Pretreatment Clinchecks (right, front, left, upper, lower).
Clincheck2: Communication with the Technician
Seven aligners later, at the follow‐up visit, we detected that the lower lateral incisor was erupting lingually, so the patient was rescanned to include its incisal edge on the aligner, so the crown could be moved to its ideal position.
The goals remained the same, therefore providing a big advantage in comparison with any other device that might have been used for the same goal, as adaptation of the new set of aligners is easy, there are no additional changes and we get a brand new set of aligners adapted to the situation.

Fig. 18.29 Refinement: (left) 32 has erupted and does not fit in the aligner; (centre) 53 has increased mobility; (right) the patient is re‐scanned and additional aligners ordered.
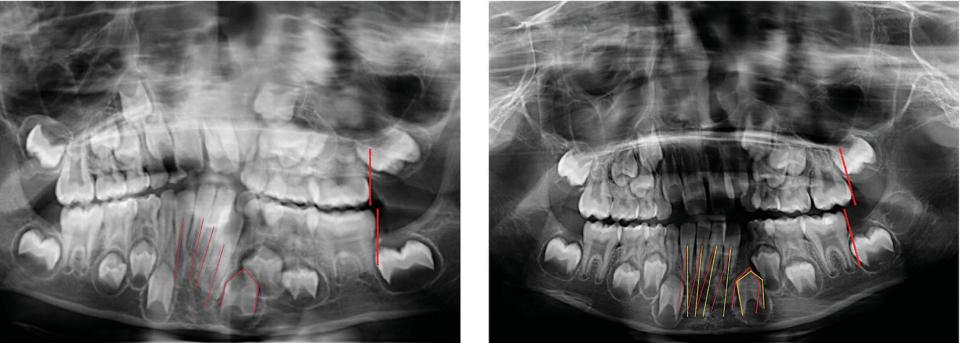
Fig. 18.30 Refinement: panoramic X‐rays show the evolution of the sagittal molar relationship on second and third quadrant, as well as improvement in lower incisor tipping, opening space for 33.

Fig. 18.31 Refinement development: Both available arch space and transverse development were achieved by distalization, proclination and expansion.
ClinCheck3: Communication with the Technician
It was discovered later that upper laterals had erupted on a cross bite, which made rescanning the patient essential to the ordering of additional aligners. The treatment plan should stay the same, except for the movement of these two teeth. The technician was asked for:
- Extrusion attachment
- Extra buccal root torque to help creating an ‘en masse’ movement that will take the apex of these two teeth to their ideal position

Fig. 18.32 Refinement: 12, 22 have erupted but their clinical crowns are not yet exposed (left), so patient is re‐scanned when clinical crowns are bigger (centre); planning an additional ClinCheck (right).

Fig. 18.33 Final Intraoral views (right, front, left, upper, lower) showing a space gain.

Fig. 18.34 Final and final smile views show an improvement in arch development.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


