Concepts of occlusion
A comprehensive discussion of occlusion is beyond the scope of this textbook. However, some fundamental concepts applicable to most dental treatments are, therefore, appropriate for esthetic dental procedures. The dental literature contains numerous definitions of specific occlusion terminology that can result in conceptual misinterpretations. Therefore this chapter uses the definitions provided in the Glossary of Prosthodontic Terms published in the 2005 Journal of Prosthetic Dentistry.1
Centric occlusion. The occlusion of opposing teeth when the mandible is in centric relation. This may or may not coincide with the maximal intercuspal position.
Maximal intercuspal position (also called maximal intercuspation). The complete intercuspation of the opposing teeth independent of condylar position sometimes referred to as the best fit of the teeth regardless of the condylar position.
Centric relation. The maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterior-superior position against the shapes of the articular eminencies. This position is independent of tooth contact. (This is a partial definition. The entire definition can be found in the Glossary of Prosthodontic Terms published in the 2005 Journal of Prosthetic Dentistry.)1
Temporomandibular joints and surrounding structures
Predictably, stable occlusion depends on proper joint mechanics and masticatory muscle activity. The joints must be evaluated for stability before any occlusal therapy. A screening evaluation should include a review of the patient’s joint history. Questions should be asked to identify any known signs or symptoms related to pain, joint noise, joint locking, limited range of movement, or trauma to either jaw joint. Further clinical testing may include joint palpation, orthopedic load testing2 (Fig. 20-2), Doppler auscultation, and joint vibration analysis.

If joints are identified with apparent intracapsular disorders, further testing through imaging may be indicated. Such joints often require stabilization therapy before initiating dental treatment. Therapy for damaged joints may include occlusal splint therapy, physical therapy, and in severe cases, joint surgery.
In complex restorative cases, centric relation may be the only reference point available to the clinician. Centric relation is precise, repeatable, and stable, in healthy joints with properly aligned condyle-disk assemblies.3 Dawson’s bilateral manipulation is one of numerous methods method of reproducing mandibular centricity.
Uniform tooth contacts
Proper occlusion refers to the simultaneous contact of both posterior and anterior teeth. This provides the following benefits:
1. It protects the joints and surrounding structures by reducing the percentage of absorbed force.4 The positioner muscles of mastication, especially the lateral pterygoids, can fully release their contraction, as the elevator muscles guide the end closure. This release of the positioner muscles protects the muscles.5
2. It protects the teeth by reducing the percentage of force through each tooth.6
Noninterfering teeth
The goal of all occlusal therapy is to position teeth so that none interfere with normal jaw function from border to border when the teeth are in occlusion. Ideally, all teeth should touch simultaneously on first contact. New restoration should not cause a shift off the arc of closure (anterior slide), the line of closure (left or right),7 or vertical hyperocclusion.
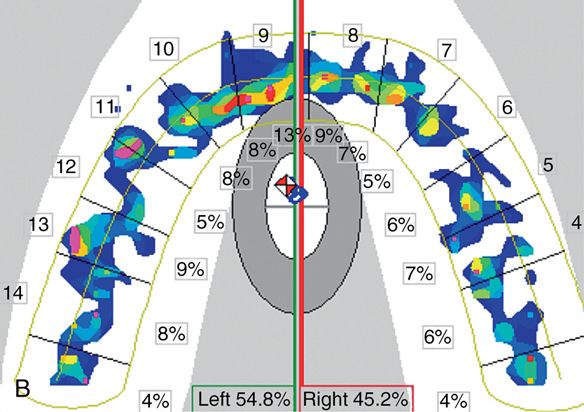
It is critical that these interferences be meticulously eliminated. Articulating ribbon is a helpful aid in identifying gross interferences, but an inconsistent quantifier of small occlusal interferences.8 Patient feedback can help to identify occlusal prematurities at the 50-μm level, half the thickness of a human hair. In certain cases the T-scan II computerized occlusal analysis (Tekscan, Boston) is helpful (Fig. 20-3). It uses a thin Mylar film containing sensors to record occlusal contacts at the micron level. This information is relayed to a computer monitor for immediate interpretation. This is the most sophisticated means of evaluating occlusal forces presently available.9

Coupled anterior teeth (Mutually protected occlusion)
Anterior coupling is a term used to designate the approximation of the maxillary and mandibular anterior teeth when the posterior teeth are at maximal intercuspation.10 It is desirable for both anterior and posterior teeth to simultaneously touch in maximal intercuspation (Fig. 20-4). This creates a sharing of occlusal forces over the maximum number of teeth on closure. It also is critical to fulfill the goal of excursive occlusal contacts, namely, immediate anterior teeth guidance and immediate posterior teeth disclusion.

“Several authors believe that mutually protected occlusion (disocclusion through anterior teeth) is ideal, since the canine teeth present higher proprioception, are ideally located (thus promoting immediate disocclusion of posterior teeth), have considerable volume and bone support and present lower electromyographic activity, i.e. they promote higher muscular relaxation, besides presenting better conditions to distribute and afford occlusal loads without harmful consequences to posterior teeth and supporting structures.”11
It is necessary for anterior teeth to couple, that is, simultaneously contact, with the posterior teeth so as to maximize physiologic health of the masticatory system.
By harmoniously sharing contact exclusively on the six anterior teeth, in all excursive movements several beneficial effects are realized:
1. The posterior teeth are protected from tooth-to-tooth-abrasive wear, harmful lateral stresses, cervical abfraction, and the damaging effects of parafunctional habits, because they are disoccluded.
2. The EMG activity of elevator muscles is significantly reduced by the disocclusiondistoclusion of the posterior teeth.12–18 Anterior teeth have a mechanical advantage over posterior teeth because they are farther from the fulcrum. This positioning gives them better leverage to offset the closing muscles of mastication. The mechanical advantage is apparent when one tries to “bite hard” with the front teeth as compared to biting hard with the molars.19–25 This has been shown to significantly reduce chronic myofascial pain in some patients.26
3. The reduction of elevator muscle force reduces the loading forces applied at the joint level.
T, D, S, F, V phonetics
When maxillary and mandibular anterior teeth are properly positioned, they will function in harmony with normal speech. T, D, S, F, and V are the strategic sounds that relate to tooth position affecting proper phonetics (Fig. 20-5).

“T” and “D” sounds are affected by the position of the lingual cingulum of the maxillary anterior teeth, from the maximal intercuspation contact to the gingival margin.27
Overcontouring or undercontouring this area can adversely affect clear phonetics. Sharp angles should be avoided.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


