Introduction
The purpose of this study was to use cone-beam computed tomography imaging to examine the skeletal and dental changes in the sagittal and vertical dimensions after rapid palatal expansion.
Methods
Twenty-eight healthy children (mean age, 9.9 years; range, 7.8-12.8 years; 17 boys, 11 girls) who required rapid palatal expansion treatment were included. For each patient, a bonded Haas-type expander with full occlusal and palatal acrylic coverage was cemented in place. Cone-beam computed tomography images were obtained as part of the pretreatment orthodontic records and at the completion of rapid palatal expansion for all patients. The mean interval between pretreatment and completion of rapid palatal expansion was 52 days (range, 19-96 days). The average skeletal age of the patients, determined from hand-wrist films also obtained before treatment, was 10.1 years. The mean expansion of the expander was 8.0 mm (range, 5.9-9.6 mm). Each cone-beam computed tomography image was compressed from the outer portion of the right side of the patient’s head to the center of the left central incisor into a 2-dimensional synthesized cephalogram, which was then traced and measured.
Results
The results showed that from pretreatment to completion of rapid palatal expansion, SNA, FH-NA, and A-Nperp increased by means of 1.04°, 0.92°, and 0.87 mm, respectively ( P <0.05). In addition, 1/-NA, 1/-SN, 1/-NA, 1/-Nperp, and 1/-PP showed mean decreases of 3.74°, 2.53°, 1.17 mm, 0.49 mm, and 2.69°, respectively ( P <0.05). Both ANS and PNS moved significantly downward (ANS, 2.05 mm; PNS, 1.16 mm).
Conclusions
There was forward movement of the maxilla as a result of rapid palatal expansion treatment. Bonded rapid palatal expansion treatment resulted in downward displacement of the maxilla with a greater displacement of ANS than PNS and posterior movement of the maxillary central incisors.
The treatment to open the midpalatal suture with rapid palatal expansion (RPE) has been widely used in orthodontics to orthopedically increase the transverse dimension of the maxilla in children. Because the palatal suture is often fused in adults, RPE becomes less effective and may produce more dentoalveolar changes rather than the desired transverse craniofacial skeletal changes.
Several studies have reported on the sagittal and vertical skeletal and dental effects of RPE on the maxilla, but their results were inconclusive. Haas and Davis and Kronman reported that the maxilla moved downward and forward with the use of Haas-type RPE. However, Silva Filho et al found that the maxilla did not change sagittally but moved downward after RPE, displaying downward and backward rotation in the palatal plane. Wertz found that the maxillary incisors were retroclined after RPE (1/-SN decreased), whereas Sandlkçloglu and Hazar reported that the maxillary incisors became more proclined (1/-SN increased). Chung and Font found that the maxilla was displaced downward and forward after RPE; however, the amount of forward movement was small and might not be clinically significant. Additionally, they found that the palatal plane was displaced downward in almost a parallel manner. Akkaya et al reported that the maxilla moved forward, and the mandible moved backward.
Previous studies regarding the effects of RPE in the sagittal and vertical dimensions focused on conventional lateral cephalograms, which are limited by factors such as magnification, superimposition of structures, and distortion caused by head position. Cone-beam computed tomography (CBCT) technology offers a reproducible 3-dimensional image without the limiting factors of magnification and distortion. Kumar et al compared cephalometric measurements from CBCT synthesized lateral cephalograms using orthogonal and perspective projections with those from conventional cephalograms and dry skulls. They found that orthogonal CBCT synthesized cephalograms provided measurements closest to the actual skull measurements and were significantly more precise than the other image modalities. These results were consistent with those of Lamichane et al, who found significant accuracy in orthogonal projections that were more representative of actual anatomy than were perspective projections. Thus, this technology inevitably results in more accurate information to examine the effects of RPE in the sagittal and vertical dimensions.
The purpose of this study was to examine the vertical and sagittal dental and skeletal effects of bonded RPE using orthogonal lateral cephalograms synthesized from CBCT.
Material and methods
This study was approved by the institutional review board of the University of Pennsylvania. Twenty-eight healthy children (mean age, 9.9 years; range, 7.8-12.8 years; 17 boys, 11 girls) who required RPE treatment at a private orthodontic practice were included in this study. The need for RPE was determined by the treating orthodontist (N.B.), and the inclusion criterion was that the patient had a maxillary transverse deficiency diagnosed from the Andrews’ 6 elements transverse analysis. No patient had either craniofacial syndromes or previous orthodontic treatment.
A pretreatment CBCT image (T1) was taken as a standard initial record for all patients. The scans were obtained with an i-CAT machine (Imaging Sciences International, Hatfield, Pa). The field of view was 22 × 16 cm, including the whole head, to provide a complete diagnosis for the patient; the voxel size was 0.4 mm; and the amount of radiation was 68 μSv. The skeletal age of each patient was determined from a hand-wrist film also obtained at T1 according to the standards of Greulich and Pyle. The mean skeletal age of the patients was 10.1 years (range, 7.3-14.8 years). For each patient, a bonded maxillary expander with full occlusal and palatal acrylic coverage was cemented in place, with coverage from the deciduous or permanent canine to the first molar. The rationale for this appliance was to have some control of the buccal tipping and eruption of the posterior teeth. The same orthodontic laboratory fabricated all expanders.
The expansion protocol consisted of 2 turns per day (0.25 mm per turn) until the required expansion (including 2 mm of overexpansion) was achieved; this was determined according to Andrews’ 6 elements transverse analysis. The amount of expansion was determined by measuring the distance between the 2 acrylic halves of the expander before and after expansion with a digital caliper. Then a postexpansion CBCT image (T2) was taken of each patient with half the amount of radiation (34 μSv) of the T1 image by reducing the imaging time from 20 to 10 seconds. The voxel size was 0.4 mm, and the field of view was 13 × 16 cm to evaluate the changes to the maxilla from RPE. The mean interval between T1 and T2 was 51.9 days (range, 19-96 days). All patients did not have brackets or wires placed in the maxillary arch until after the T2 records were taken.
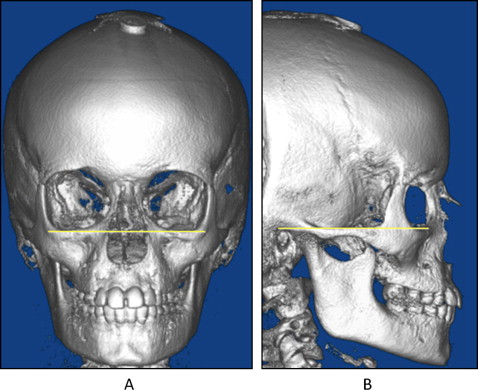
All CBCT images were oriented and standardized using Dolphin Imaging software (version 10.5; Dolphin Imaging & Management Solutions, Chatsworth, Calif). Each head was oriented by the frontal and lateral views. In the frontal view, the head was oriented with the floor of the orbits parallel to the floor; in the right lateral view, the Frankfort horizontal line was parallel to the floor ( Fig 1 ).
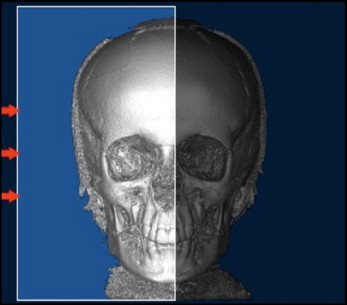
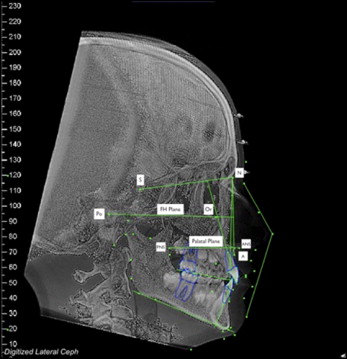
Each image was compressed from the outer portion of the right side of the patient’s head to the center of the left central incisor into a 2-dimensional orthogonal projection ( Fig 2 ). Then the CBCT-synthesized cephalograms were built using orthogonal projections. The definition of the landmarks corresponded to those given by Riolo et al. Each image was traced by 1 examiner (M.H.) and verified by an orthodontic professor (C.-H.C.). Both examiners agreed on all cephalometric landmarks. To minimize tracing errors, the lateral cephalograms at T1 and T2 were superimposed on the cranial base to match the landmarks of porion and orbitale. The following measurements were made ( Fig 3 ).
- 1.
Sagittal skeletal: SNA angle (in degrees), Frankfort horizontal plane to NA angle (FH-NA, in degrees), and A-N perpendicular (A-Nperp, in millimeters). Increases in angular measurements were considered positive, and decreases were considered negative. For the linear measurements, forward displacement of the skeletal structure from T1 to T2 was given a positive value, whereas backward displacement was considered negative.
- 2.
Sagittal dental: 1/NA (in degrees and millimeters), 1/SN (in degrees), 1/-Nperp (in millimeters), and 1/-PP (in degrees). Increases in angular measurements from T1 to T2, indicating maxillary incisor proclination, were considered positive; decreases in angular measurements, indicating incisor retroclination, were considered negative. For the linear measurements, forward movement of the maxillary incisor was considered positive, and posterior movement was considered negative.
- 3.
Vertical: anterior nasal spine (ANS) difference (in millimeters) and posterior nasal spine (PNS) difference (in millimeters). The values of these differences were calculated by superimposing the lateral cephalograms (T1 and T2) on the anterior cranial base and measuring the distance between the positions of ANS and PNS at T1 and their positions at T2. The difference was considered positive if ANS and PNS moved downward from T1 to T2, and negative if ANS and PNS moved upward from T1 to T2.
All tracings, measurements, and data were completed by the same examiner (M.H.) and verified by the same orthodontic professor (C.-H.C.). All data were tested for reliability and reproducibility by conducting intraexaminer trials. To test intraexaminer reproducibility, 14 patient records were randomly selected, reoriented, retraced, and remeasured by the same examiner and compared with the original measurements. A paired Student t test was used to determine whether there was a significant difference between the 2 measurements taken at the 2 times.
Descriptive statistics including means, standard deviations, and ranges were calculated for the measurements at T1 and T2. A 2-tailed Student t test was used to determine whether there was a difference in the measurements from T1 to T2. The significance was predetermined at P <0.05.
Results
The intraexaminer reproducibility test showed that only 1 (1/-NA [mm]) of the 10 measurements had significant differences ( P <0.05) between the original data set and the data set that was remeasured. However, the Pearson correlation coefficient for all measurements varied between 0.99 and 0.97. Therefore, the measurements in this study were highly reproducible and reliable.
The mean amount of expansion measured from the expander was 8.0 ± 0.8 mm (range, 5.9-9.6 mm).
Table I details the sagittal skeletal effects from the data. SNA, FH-NA, and A-Nperp increased by means of 1.04°, 0.92°, and 0.87 mm, respectively, after RPE. All 3 measurements were statistically significant at P <0.05.
| n | Mean difference from T1 to T2 | SD | Range | P value | |
|---|---|---|---|---|---|
| SNA (°) | 28 | +1.04 | 1.1 | −1.2 to +5.1 | <0.05 ∗ |
| FH-NA (°) | 28 | +0.92 | 1.41 | −1.7 to +4.6 | <0.05 ∗ |
| A-Nperp (mm) | 28 | +0.87 | 1.97 | −0.9 to +4.2 | <0.05 ∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


