Introduction
The aim of this prospective cohort study was to compute the clinical survival and complication rates of a miniplate with a tube device (C-tube) used for orthodontic treatment.
Methods
From August 2003 to May 2012, 217 patients were recruited. They received 341 C-tube miniplates. Some C-tube miniplates were removed because orthodontic treatment ended. Others remained beyond the study period and were recorded as censored data. Survival was classified as a C-tube miniplate that functioned in the mouth regardless of any complications. Success was defined as survival without complications. From the data, the effects of these clinical variables on the survival of the C-tube miniplates were evaluated: sex, age, jaw, placement sites, oral hygiene, tube clearance, inflammation, miniplate shape, number of screws, and length of the fixation screws. Survival analyses using the Kaplan-Meier method and the Cox proportional hazard model were applied.
Results
Of the 341 miniplates, 14 failed, and 32 had complications. Two-year survival and success rates were 0.91 and 0.80, respectively. In terms of the simple ratio statistic, this was equivalent to a success rate of 96%. The status of oral hygiene maintenance and the operators’ experience had significant associations with the complication rates ( P <0.001).
Conclusions
The C-tube miniplate has an advantage in versatility in terms of force application. When placing a miniplate, the most important factor is maintaining good tissue health by means of good oral hygiene. Even with good hygiene, the doctor’s experience in performing the flap surgery was the second most important factor for success.
The orthodontic miniplate system was initially similar to the maxillofacial plating system, which evolved to have a specifically modified end to engage orthodontic auxiliaries. Recently, orthodontic miniplate systems have become increasingly accepted by both patients and clinicians as a safe and effective adjunct for complex orthodontic treatment. Some attachments can also be added onto the miniplate. A miniplate with a tube device, such as a C-tube or a Bollard miniplate implant, is an efficient tool for borderline patients who would have been otherwise difficult to treat.
Clinicians are frequently concerned about the ultimate success rate and the risk factors involved in miniplate failures and complications. The most conspicuous findings when comparing miniplates with mini-implants are the better stability and higher success rates of miniplates. Despite their popularity, orthodontic mini-implants have failure rates as high as 10% to 24%. However, miniplate failure rates vary from 1% to 7%.
Survival analysis is a systematic statistical method of evaluating the mechanical success or failure of a particular system. Survival analysis has several advantages of measuring a failure pattern over time, especially when those survival data have a principal end point. Most orthodontic articles have reported simple success or failure rates of mini-implants, but some have used survival analysis when evaluating mini-implant success or failure. However, a survival analysis has not yet been used to analyze the long-term success or failure of miniplates. Reports of the success or failure patterns of miniplates over time have been missing from the literature. Even in what has been categorized as clinical success, miniplates sometimes cause complications such as swelling, tissue proliferation, and infection, which can lead to loosening of the miniplate. These adverse complications are not reflected in a simple success or failure rate. A better analysis that distinguishes among simple survival of the miniplate and success with or without various complications would provide valuable guidelines to a clinician wishing to use miniplates and maximize their clinical conditions.
The aim of this prospective cohort study was to analyze the clinical survival and success rates without complications of the miniplate and tube device used for orthodontic treatment.
Material and methods
All patients were treated with fixed appliances. The miniplate with a tube device (C-tube; Jin Biomed, Bucheon, Korea) used for this clinical study was composed of a titanium miniplate fixture on the bone side and a welded tube on the oral cavity side. The subjects included 217 patients (137 female, 80 male; average age, 22 years; range, 11-61 years) who had undergone orthodontic treatment with a C-tube miniplate ( Fig 1 ). From August 2003 through May 2012, the subjects were treated at 3 university-affiliated hospitals by 3 orthodontists, who performed their plate placement surgeries. The institutional review board for the protection of human subjects reviewed and approved the research protocol (KHD IRB-1208-02).
The surgical procedure for placing the C-tube was the following. As a chairside procedure under local anesthesia, all miniplates were placed by 3 orthodontists. After local anesthesia and palpation of the surgical area, a 5-mm vertical incision was made. The periosteum was detached with an elevator. The C-tube miniplate was positioned with the tube-shaped head remaining exposed to the oral cavity and then anchored with 2 to 4 titanium screws (diameter, 1.5 mm; length, 4-6 mm). One or 2 sutures were placed after fixation of the miniplate. More detailed information of the miniplate placement and removal was discussed in previous articles.
A total of 341 C-tube miniplates were examined in this study. These clinical variables were investigated: sex, age, jaw, placement sites, oral hygiene, tube clearance, inflammation, miniplate shape, number of screws, and length of screws. The appropriate dimensions of the miniplate (plates with 2, 3, or 4 holes) were selected according to the bone screw length, soft-tissue height, position and shape of adjacent teeth, and placement site in the oral cavity. After a 1- to 2-week period of healing for the device, the tube part was loaded with the desired orthodontic force.
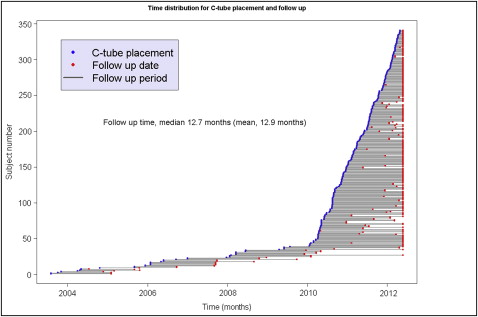
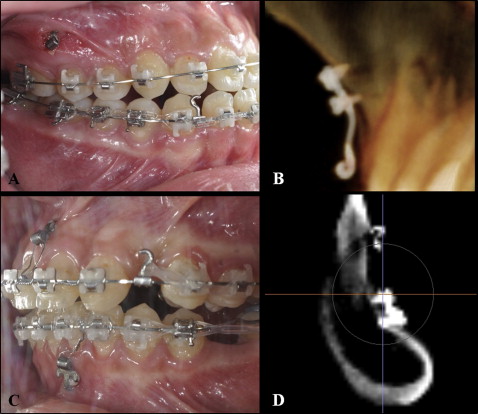
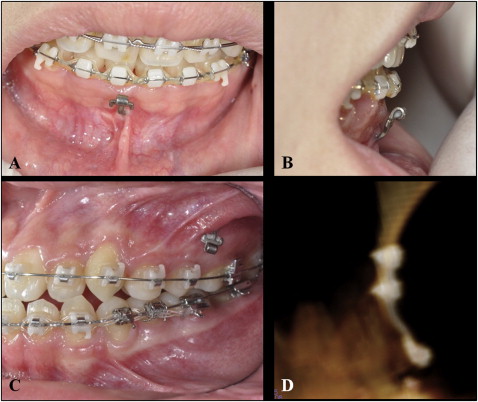
We used survival analysis to evaluate the reliability of the C-tube miniplates as anchorage for fixed orthodontic treatment. Survival time was coded by the number of months after placement of the miniplate. Failure was defined when a miniplate had to be removed because of loosening, loss of attachment, or infection and was coded as event data ( Fig 2 ). For subjects whose follow-up times ended without a failure event, the end status was recorded as “censored” because the actual time to a failure event was considered to be unknown, since the miniplate had not yet failed before the end of orthodontic treatment ( Fig 3 ). To restate, the intact C-tube miniplate that was functioning properly during and beyond the orthodontic treatment period was coded as censored. Complications were coded for tissue irritation, screw loosening, screw fracture, or localized and transient inflammation. Survival was classified as a tube on a miniplate that functioned in the mouth regardless of any of these complications. Success was defined as survival without any complication.
Statistical analysis
The Fisher exact test significance and odds ratio statistics were calculated. Kaplan-Meier survival curves were plotted, and the log rank test was used to identify the variables associated with the failures. Prognostic variables were identified with the Cox proportional hazard model. The R programming language was used for the data analysis. A P value less than 0.05 was considered statistically significant.
Results
The average follow-up period was 12.9 months (median, 12.7 months) and ranged from 2 weeks to 4.3 years ( Fig 1 ). Table I shows the coded events that occurred in this study. During the study, 14 C-tube miniplates were removed before the end of treatment. Thirty-two plates had complications such as transient abscess, tissue irritation, loosening, or screw fracture. Among the 32 C-tube miniplates with complications, 18 plates were capable of functioning throughout the orthodontic treatment time.
| Coded events | Number of C-tube miniplates |
|---|---|
| Total | 341 |
| Failure | 14 |
| Detachment | 9 |
| Loosening | 2 |
| Abscess | 1 |
| Tissue irritation | 1 |
| Wrong direction | 1 |
| Survival ∗ | 327 |
| Complications | 32 |
| Loosening (loosened but functioned) | 8 |
| Abscess (transient and subsided) | 1 |
| Tissue irritation (transient and subsided) | 8 |
| Screw fracture (screw removed) | 1 |
| Success † | 309 |
∗ Survival equals the total with any complication minus the failures.
Among the investigated clinical variables, sex, age, jaw, placement site, and number of screws had no significant effect on the survival of the tube and the plate. Table II shows the results of conventional ratio tests for the effects of the clinical variables on the complications. Oral hygiene, tissue condition, shape of the miniplate, length of the screws, and operator factor had significant associations with the complication rate. As previously mentioned, the use of survival analysis, depicted by Kaplan-Meier curves, allows for a more informative analysis of failures and successes, instead of simply reporting the ratios. The Kaplan-Meier survival curve with the log rank test agreed with the aforementioned ratio test results. In addition, the Kaplan-Meier survival curves showed that the cumulative 2-year survival and success rates were 0.91 and 0.80, respectively. One-year survival and success rates were 0.96 and 0.92, respectively ( Table III ). In terms of the simple and conventional ratio statistic, the overall success rate was 96%, as shown in Table II .
| Variable | Censored (n) | Failures (n) | Complications (n) † | Total (n) ‡ | P value ∗ | Odds ratio (95% CI) |
|---|---|---|---|---|---|---|
| Sex | 0.261 | |||||
| Male | 122 | 5 | 16 | 203 | 1 | |
| Female | 187 | 9 | 16 | 138 | 0.7 (0.7, 3.4) | |
| Age (y) | 0.357 | |||||
| <20 | 154 | 6 | 13 | 167 | 1 | |
| >20 | 155 | 8 | 19 | 174 | 1.5 (0.7, 3.3) | |
| Jaw | 0.578 | |||||
| Maxilla | 164 | 7 | 15 | 179 | 1 | |
| Mandible | 145 | 7 | 17 | 162 | 1.3 (0.6, 2.9) | |
| Placement site | 0.837 | |||||
| Anterior | 87 | 6 | 8 | 95 | 1 | |
| Posterior | 222 | 8 | 24 | 246 | 1.2 (0.5, 3.2) | |
| Oral hygiene | <0.001 | |||||
| Good | 286 | 4 | 12 | 298 | 1 | |
| Poor | 23 | 10 | 20 | 43 | 20.7 (8.3, 52.0) | |
| Tube clearance | 0.379 | |||||
| Exposed | 276 | 11 | 27 | 303 | 1 | |
| Covered | 33 | 3 | 5 | 38 | 1.6 (0.4, 4.5) | |
| Tissue condition | <0.001 | |||||
| Good | 254 | 6 | 14 | 268 | 1 | |
| Inflammation | 55 | 8 | 18 | 73 | 5.9 (2.6, 13.7) | |
| Miniplate shape | 0.039 | |||||
| I-bar | 248 | 12 | 20 | 268 | 1 | |
| T-bar | 61 | 2 | 12 | 73 | 2.4 (1.0, 5.6) | |
| Screws (n) | 0.073 | |||||
| 1 or 2 | 263 | 13 | 23 | 286 | 1 | |
| >2 | 46 | 1 | 9 | 55 | 2.2 (0.9, 5.4) | |
| Length of screws (mm) | 0.027 | |||||
| ≤4 | 161 | 6 | 10 | 171 | 1 | |
| ≥5 | 148 | 8 | 22 | 170 | 2.4 (1.0, 5.8) | |
| Patient sources and operators | 0.005 | |||||
| A | 162 | 6 | 8 | 170 | 1 | |
| B | 92 | 6 | 12 | 104 | 2.6 (1.0, 7.7) | |
| C | 55 | 2 | 12 | 67 | 4.4 (1.6, 13.1) |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


