34 Distant Metastases and Management
Basic Mechanisms of Metastasis
TP53 and Other Apoptosis-Related Genes
Vascular Endothelial Growth Factor
Clinical Features and Pathological Aspects
Frequency of Distant Metastases
Carcinoma Ex Pleomorphic Adenoma
Metastasizing Pleomorphic Adenoma
Surgery for Distant Metastases
Introduction
Metastasis is the most insidious and life-threatening aspect of the natural history of malignant tumors. Despite improvements in early diagnosis, surgical techniques, general patient care, and local and systemic adjuvant therapies, most deaths in cancer patients result from the relentless growth of metastases. In general, distant metastases from carcinoma arising in the head and neck region are considered to be infrequent. However, in patients affected by carcinomas of the major salivary gland, the incidence of failures at distant sites is higher, giving rates as high as 20%–50%, depending on different histotypes, and thus still representing the main cause of death. These figures are difficult to improve, mainly because studies attempting to clarify the clinicopathological and molecular aspects of distant spread in salivary gland carcinomas are hampered by the uncommon occurrence of the lesions and by the fact that more than a decade of observation may be required to appreciate their prolonged clinical course.
In this chapter, we review current knowledge about the mechanisms implicated in the development of salivary gland tumor metastases, as well as their clinicopathological features, with an emphasis on possible medical and surgical treatments for this disease.
Basic Mechanisms of Metastasis
The molecular mechanisms behind the development of metastases are poorly understood, largely because tumor metastasis is a complex process involving several distinct steps. These include the escape from the primary tumor, dissemination through the circulation, lodgment in small vessels at distant sites, penetration of the vessel wall, and growth in the new site as a secondary tumor. Other limiting factors to be considered in the metastatic process are the acquisition of a vascular supply via the process of neoangiogenesis or through cooption of preexisting vessels, and the acquisition of resistance to apoptosis to survive after detachment from matrix substrates and during dissemination and colonization of ectopic sites. This is accomplished through the deregulation of several molecular pathways, which can be studied at the genomic (genetic and epigenetic), transcriptional, translational, and post-translational levels.
With regard to salivary gland carcinomas, a major limitation on our comprehension of these mechanisms has been the rarity of the disease, which together with the wide range of histological types and variability of clinical behavior has hindered the gathering of clinically relevant data. Different approaches have been used to study the molecular basis of the process of metastasis in salivary gland cancer. Earlier studies mainly focused on analyzing single factors possibly implicated in the development of metastases, while more recently high-throughput genomic and proteomic analyses have been successfully employed.
 Owing to the rarity of salivary gland cancer, knowledge about the special characteristics of the metastatic process in this cancer type is very limited.
Owing to the rarity of salivary gland cancer, knowledge about the special characteristics of the metastatic process in this cancer type is very limited. E–Cadherin
E–Cadherin
The cellular activities implicated in the early phases of the metastatic process are cell–cell adhesion, cell–matrix adhesion, proteolysis, migration, survival, and growth. Epithelial (E)-cadherin, a transmembrane glycoprotein of the type I cadherin superfamily, is a key molecule implicated in cell-to-cell adhesion. It binds to the cytoskeleton through the catenin molecules, and this complex maintains the structure of the epithelium by homophilic (E–cadherin to E–cadherin), homotypic (epithelial cell to epithelial cell) adhesion. Loss of E–cadherin favors the invasion process, as confirmed by several in vitro and in vivo models. With regard to salivary gland carcinomas, we showed for the first time that in adenoid cystic carcinoma, loss of differentiation from a tubular to a cribriform to a solid pattern is accompanied by loss of E–cadherin expression.1 In addition, tumors with low or absent expression of the adhesion molecule more frequently had distant metastases and behaved more aggressively, with shorter disease-free and overall survival periods. Subsequent studies have shown that reduced E–cadherin levels are more often due to promoter methylation.2 Abnormal expression of E–cadherin and α–catenin has also been frequently observed in mucoepidermoid carcinoma.3
 Reduced E–cadherin expression in salivary gland cancer correlates with a higher frequency of distant metastases.
Reduced E–cadherin expression in salivary gland cancer correlates with a higher frequency of distant metastases.
 Integrin Family
Integrin Family
The integrins are another family of cell surface molecules that have been implicated in tumor invasion and metastasis. They are noncovalent heterodimeric membrane complexes consisting of an α and a β subunit. Currently, 18 different α subunits, three β subunits, and 24 heterodimers have been identified in mammals. Analysis of their expression in salivary gland carcinomas has shown a reduction of the α chain in carcinomas in comparison with adenomas.4 However, in vitro studies did not show any significant differences in integrin expression between an adenoid cystic carcinoma cell line with a low metastatic tendency and one with highly metastatic behavior.5
 Matrix Metalloproteinases
Matrix Metalloproteinases
Another crucial step for cancer invasion and metastasis is matrix metalloproteinase (MMP)–mediated degradation of the extracellular matrix, which is balanced by the activity of the tissue inhibitors of metalloproteinase (TIMPs). Different approaches have been used to assess the presence of MMPs and TIMPs and their possible significance in salivary gland cancer. Analysis of the production levels of eight different MMPs (MMP-1, -2, -3, -7, -8, -9 and -13, and MT1-MMP) and two tissue inhibitors of metalloproteinases (TIMP-1 and -2) in homogenates of human salivary gland carcinomas suggested that enhanced activation of pro-MMP-2 mediated by MT1-MMP is implicated in invasion and metastasis by mucoepidermoid carcinoma, and that TIMP-2 may regulate pro-MMP-2 activation in salivary gland carcinomas.6 In another study using an immunohistochemical approach, significantly higher levels of MMP-2 were detected in carcinomas in comparison with adenomas, indicating that MMP-2 expression in particular may be related to the invasive properties and the malignant potential of these tumors.7 In addition, TIMP expression correlates with the growth pattern of the tumor, as indicated by studies conducted in adenoid cystic carcinoma, where the expression of TIMP-1 and -2 decreased in the cribriform pattern in comparison with the tubular pattern.8 Finally, an attempt has been made to evaluate the prognostic significance of MMPs in salivary gland carcinomas, and overexpression of MMP-13 appears to be associated with poor survival in acinic cell carcinoma, while high levels of MMP-9 predicted a poor prognosis in adenoid cystic carcinoma and salivary duct carcinoma.9 Overall, these studies indicate a disturbed balance between MMP and TIMP in malignant salivary gland tumors, which could be a relevant factor in the development of distant metastases—although the data are too few and too fragmented for any definitive conclusion to be drawn.
 TP53 and Other Apoptosis-Related Genes
TP53 and Other Apoptosis-Related Genes
In the process of metastatic dissemination, tumor cells have to detach from the surrounding matrix or from neighboring cells. In normal conditions, epithelial cells undergo apoptosis (programmed cell death) when adhesion to the correct substrate is disrupted, and metastatic cells therefore need to be resistant to apoptosis in order to survive during dissemination and colonization of ectopic sites. Apoptosis is modulated by several genes, including BCL2 (B–cell CLL/lymphoma 2) and its related genes, TP53 (tumor protein p53), RB1 (retinoblastoma 1), and MYC (v-myc myelocytomatosis viral oncogene homolog). BCL2 acts as an antiapoptotic regulator, and one might therefore expect increased expression of it in high-grade salivary carcinomas; however, this has not been the case in the studies conducted so far.10
Conversely, inactivation of TP53 appears to correlate with increased aggressiveness in salivary gland carcinomas. We have demonstrated that aberrations in p53 oncoprotein were statistically associated with regional and distant metastases and that patients whose cancers had moderate or high p53 protein expression had lower disease-free and actuarial survival rates than those with low or wild-type p53 expression.11
 As in other head and neck cancer types, inactivation of TP53 is associated with more aggressive salivary gland cancer.
As in other head and neck cancer types, inactivation of TP53 is associated with more aggressive salivary gland cancer.
 RUNX3
RUNX3
Runt-related transcription factor-3 (RUNX3) is a tumor-suppressor gene that plays an important role in inhibiting cellular growth by participating in transforming growth factor-β–dependent apoptosis. In a study of RUNX3 expression in adenoid cystic carcinoma, it was shown that tumors with low RUNX3 expression were biologically more aggressive and at increased risk of distant metastasis, leading to a fatal outcome—supporting a possible involvement of this gene in the metastatic process.12
 Vascular Endothelial Growth Factor
Vascular Endothelial Growth Factor
Tumor growth and progression is limited before the neoplastic mass becomes vascularized. The process of (neo)-angiogenesis makes tumor growth possible and creates leaky capillaries, which can serve as conduits for disseminating cells. As observed in several tumor types, increased angiogenesis is associated with a poorer prognosis and with distant metastases in major subtypes of salivary gland carcinoma.13,14 According to these studies, vascular endothelial growth factor (VEGF) appears to play a major role as a proangiogenic molecule in mucoepidermoid and adenoid cystic carcinomas.
Interestingly, VEGF receptors, as well as epidermal growth factor receptor, represent potential targets for therapy in salivary adenoid cystic carcinoma. Treatment with AEE788, a dual inhibitor of endothelial growth factor (EGF) and VEGF receptor (VEGF–R) tyrosine kinases, inhibited tumor growth and prevented lung metastasis in an in vivo model, inducing a reduction in microvessel density, associated with a decrease in the level of matrix metalloproteinase-9 and matrix metalloproteinase-2 expression.15
 Factors implicated in the development of distant metastases in salivary gland tumors include:
Factors implicated in the development of distant metastases in salivary gland tumors include:
 Adhesion molecules: ↓ E–cadherin, ↓ integrin
Adhesion molecules: ↓ E–cadherin, ↓ integrin
 Matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs): ↑ MMP-2, ↓ TIMP1 and TIMP2
Matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs): ↑ MMP-2, ↓ TIMP1 and TIMP2
 Tumor suppressor genes: ↑ p53 expression, ↓ RUNX3
Tumor suppressor genes: ↑ p53 expression, ↓ RUNX3
 Angiogenesis: ↑ VEGF
Angiogenesis: ↑ VEGF
 Genomics and Proteomics
Genomics and Proteomics
A deeper understanding of the mechanisms implicated in the development of distant metastases requires expression analysis of multiple genes or proteins simultaneously. This has recently been made possible by gene expression array and proteomics analyses, which are making an important contribution to our understanding of the molecular basis of metastasis and have provided promising prognostic and predictive information by making it possible to identify which tumor will or will not metastasize. Huang and co-workers16 used the cDNA microarray technique to examine differences in gene expression profiles between the salivary adenoid cystic carcinoma cell line ACC-2 and a highly metastatic salivary adenoid cystic carcinoma clone, ACC–M. They assumed that since ACC-2 and ACC–M share an identical genetic background except for different metastatic behavior, the differentially expressed genes could be regarded as metastasis-related genes, playing direct or indirect roles in the development of metastasis. In this study, 30 genes were found to be differentially expressed, 18 of which were up-regulated and 12 down-regulated. Some of these genes are well-known metastasis-related genes and are involved in immune surveillance, cell–cell and cell–matrix interactions, signaling pathways, and growth control.
In the same in vitro model, proteomic analysis based on two-dimensional gel electrophoresis and mass spectrometry was used to determine the protein profiles associated with tumor metastasis.17 Twelve protein spots showed significant quantitative and qualitative variations, and some of the proteins identified showed associations with distinct aspects of tumor metastasis.
High-throughput analysis of differentially expressed genes and proteins will therefore in the near future be able to provide the basis for rationally determining which pathways are appropriate for further study and which molecular targets may be potentially useful for targeted therapy in patients with salivary gland carcinoma.
 To date, the results of genomic and proteomic analyses of salivary gland cancers are still too preliminary for them to have a direct impact on the treatment and prognosis of salivary gland cancer.
To date, the results of genomic and proteomic analyses of salivary gland cancers are still too preliminary for them to have a direct impact on the treatment and prognosis of salivary gland cancer.
Clinical Features and Pathological Aspects
 Frequency of Distant Metastases
Frequency of Distant Metastases
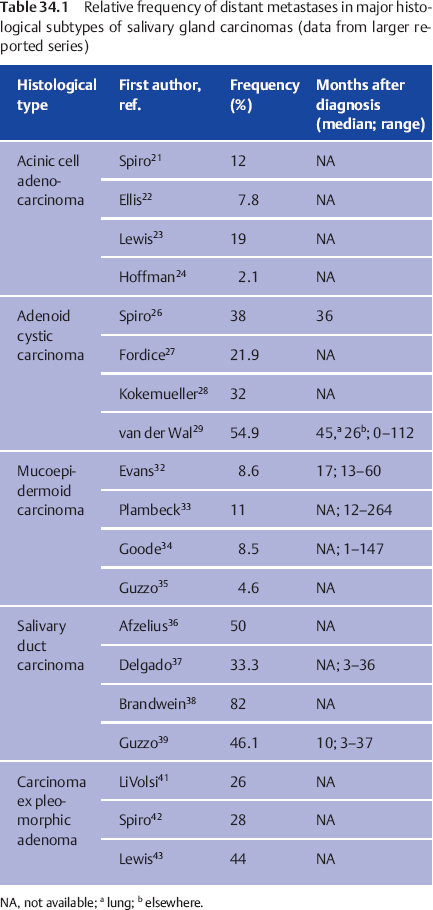
In general, the frequency of distant metastases in salivary gland carcinomas varies between 12% and 28%, according to the literature reports,18 but there are important differences depending on the histological subtypes. These can be grouped into low-grade and high-grade, and this reflects the biological behavior of the tumor—although the distinction is not always predictive, especially in some tumor types. In addition, depending on the location of the primary lesion, tumors of the tongue and submandibular gland are associated with highest rates of distant metastases.19,20 Table 34.1 summarizes the literature data on the relative frequency of distant metastases in the major histopathological categories.
 Acinic Cell Carcinoma
Acinic Cell Carcinoma
The incidence of distant metastases in acinic cell adenocarcinoma varies widely in different series, but the average rate of metastases detected at presentation and during the follow-up is around 15%.21–24 Notably, metastases and tumor-related deaths may occur several years after the initial treatment, with late deaths being recorded 38 years after diagnosis.24 Metastases mainly involve the lungs and bones. No predictive clinical or pathological parameters have so far been identified. A rare but ominous event is high-grade transformation of conventional acinic cell carcinoma, which is defined as the histological progression of a low-grade malignant neoplasm to a high-grade one, usually appearing histologically as a solid, undifferentiated carcinoma within which the original line of differentiation is lost. Acinic cell carcinoma with high-grade transformation has a poor clinical outcome, as it tends to recur, shows perineural and angiolymphatic intravascular invasion, and has a clinical course that is fatal in most cases, with frequent distant dissemination and tumor-related death.25
 Adenoid Cystic Carcinoma
Adenoid Cystic Carcinoma
Adenoid cystic carcinoma is a rare and highly lethal cancer characterized by a protracted natural course, with a significant propensity for late distant metastases, which can cause death even decades after definitive treatment.26–29 It has a predilection for hematogenous spread to lungs, bones, brain, and viscera. The presence of a solid architecture is associated with a more aggressive clinical course, although no predictive value for distant spread was observed in a large series.30 Tumor size larger than 3 cm, locoregional recurrence, and cervical node involvement were identified as predictors of distant metastases in a study of 196 patients.26 With regard to acinic cell adenocarcinoma, the onset of a high-grade undifferentiated carcinoma within an otherwise typical adenoid cystic carcinoma is accompanied by an increase in the tumor’ s aggressiveness and rapid development of regional and distant metastases.31
 Mucoepidermoid Carcinoma
Mucoepidermoid Carcinoma
With regard to mucoepidermoid carcinoma, most authors agree that its behavior is largely dependent on the histological grade. In general, metastases develop in 5%–10% of patients, almost always affected by high-grade tumors, while they are only sporadically observed in low-grade tumors.32–35 Hematogenous spread is often associated with or preceded by locoregional recurrence.
 Salivary Duct Carcinoma
Salivary Duct Carcinoma
Salivary duct carcinoma is a rare high-grade tumor that has a striking similarity to ductal carcinoma of the breast. The tumor has rapid growth, with relatively frequent facial nerve impairment, frequent locoregional spread, and a rate of distant metastasis of over 50%, with involvement of lung, bone, liver, kidney, and brain.36–39 Patients with local recurrence and/or with positive lymph nodes have the worst outcome.40
 Carcinoma Ex Pleomorphic Adenoma
Carcinoma Ex Pleomorphic Adenoma
With regard to carcinoma ex pleomorphic adenoma, most authors have found that the extent of invasion correlates with the outcome, with an excellent prognosis in tumors in which the carcinoma component is confined within the pleomorphic adenoma (intracapsular) or shows minimal invasion.41 Conversely, widely invasive tumors are associated with relatively poor survival, with a rate of distant metastases ranging between 26% and 44%.41–43 According to these series, the risk for distant spread is higher following local recurrence of the tumor.
 Metastasizing Pleomorphic Adenoma
Metastasizing Pleomorphic Adenoma
Metastasizing pleomorphic adenoma is a distinctive entity that should be kept separate from true carcinoma ex pleomorphic adenoma. It can be defined as a lesion histologically identical to pleomorphic adenoma, which inexplicably develops local or distant metastases. In the largest series reported so far, the primary lesion was in most cases located in the parotid gland.44 Most patients suffered two or more recurrences before the development of metastatic foci, and this suggests that surgical procedures and multiple recurrences may facilitate the entry of neoplastic cells into the blood vessels. Metastases have been discovered 6–52 years after the occurrence of the primary lesion, and they involved the bone, lung, regional lymph nodes, skin, kidney, retroperitoneum, oral cavity, pharynx, calvaria, and central nervous system. Two patients (18%) died as a direct result of metastatic tumor at 3 and 2 years after metastasis of their pleomorphic adenoma. So far, chromosomal abnormalities that might be related to the development of a metastatic phenotype have been described in only one case,45 while other predictors of metastatic behavior in pleomorphic adenoma have not been identified. It has therefore been suggested that metastasizing pleomorphic adenoma can be regarded as a low-grade, potentially lethal malignant disease that may involve submicroscopic malignant transformation, with molecular-genetic alterations.46
 Personal Data
Personal Data
We report here on the relative frequency of distant metastases relative to several histopathological and clinical parameters in a series of 165 consecutive parotid cancer patients treated at our institution in the period 1970–1999. The distribution by histological subtype and the frequency of distant metastasis for each subtype are shown in Table 34.2. The overall incidence of distant metastases in the series was 23.6%, and metastasis was the first site of failure in 25.7%. Overall, however, patients who experienced a distant failure represented 76.4% of those who died of the disease, suggesting that distant control represents a major problem in parotid gland cancer.
|
Histological type |
Patients (n) |
Metastases n (%) |
|
Adenoid cystic carcinoma |
40 (24.2%) |
9 (22.5%) |
|
Mucoepidermoid carcinoma |
37 (22.4%) |
5 (13.5%) |
|
Acinic cell carcinoma |
30 (18.2%) |
5 (16.7%) |
|
Carcinoma ex pleomorphic adenoma |
17 (10.3%) |
7 (41.2%) |
|
Squamous cell carcinoma |
12 (7.3%) |
3 (25%) |
|
Adenocarcinoma not otherwise specified |
10 (6.1%) |
3 (30%) |
|
Salivary duct carcinoma |
9 (5.5%) |
4 (44.4%) |
|
Undifferentiated carcinoma |
7 (4.2%) |
3 (42.9%) |
|
Myoepithelial carcinoma |
2 (1.2%) |
0 |
|
Epithelial–myoepithelial carcinoma |
1 (0.6%) |
0 |
|
Total |
165 (100%) |
39 (23.6%) |
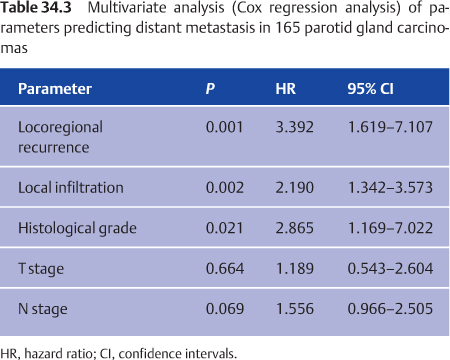
Kaplan–Meier analysis of metastasis-free survival showed that T stage, signs of local aggressiveness (including facial nerve invasion and invasion of adjacent tissues), local recurrence, lymph-node metastases, and clinical stage among the clinical parameters, and grade among the histological parameters, were significantly related to the occurrence of distant metastases. Multivariate Cox proportional hazard analysis taking all of the above-mentioned variables into account showed that signs of local aggressiveness, local recurrence, and histological grade were independent predictors of distant metastases (Table 34.3).
The analysis indicates that high-grade carcinomas are associated with a metastatic rate that is approximately three times that of low-grade carcinomas (30.3% versus 10.7%; P = 0.006 with Fisher’s exact test). Spread to distant sites tends to occur within the first 2 years after diagnosis in low-grade carcinomas, while metastases continue to occur even after 10 years in high-grade tumors.
Tumor data from clinical findings and from laboratory animals clearly show that when there is local failure after the initial treatment (surgery plus radiotherapy) of their primary tumor, there is a higher incidence of distant metastases than when local control is maintained. This has been reported for a wide range of tumor types and anatomic sites, including squamous cell carcinoma of the head and neck. If this were also true for parotid gland cancer, then more successful treatment for the primary disease would also yield increased survival rates due to the reduced risk of distant failures. In a previous study, we reported on the lack of correlation between locoregional failure and the occurrence of distant metastases in a series of 124 consecutive parotid gland cancer patients,47 suggesting different biological behavior in salivary gland carcinoma from other cancers of the head and neck area. However, a larger series with an extended follow-up period did not confirm this observation, because here we observed that patients who experienced locoregional recurrences had a significantly shorter interval to metastases and that the number of patients who developed distant metastases was significantly higher in the group of patients who experienced locoregional recurrence (35.7%) than in the group of patients who remained locally disease-free (17.4%; P = 0.02 with Fisher’s exact test).
 The clinical and histological risk factors for distant metastasis from salivary gland cancer do not differ from those in other types of head and neck cancer: T stage, signs of local aggressiveness (including facial nerve invasion and invasion of adjacent tissues), local recurrence, N stage, and histological grading.
The clinical and histological risk factors for distant metastasis from salivary gland cancer do not differ from those in other types of head and neck cancer: T stage, signs of local aggressiveness (including facial nerve invasion and invasion of adjacent tissues), local recurrence, N stage, and histological grading.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


