An 8-year-old Chinese girl sought treatment for a severe skeletal Class III malocclusion and open-bite skeletal pattern. Traditionally, patients with a skeletal Class III malocclusion are treated after they have stopped growing, and then they are treated with a combined orthodontic and orthognathic surgery approach. But the risks and expenses of this treatment plan are not acceptable to all patients. This young patient was treated with facemask therapy, a maxillary expansion device, and a molar occlusal splint for maxillary developmental stimulation with control of vertical jaw growth. After the completion of orthopedic therapy, 2 × 4 technology was used to adjust molar positions. A bonded tongue crib was used in the early permanent dentition to help the patient break her bad tongue habits. Straight-wire appliances were used for 16 months to adjust the occlusal relationship. This achieved significant improvement in anterior tooth relationships and facial profile esthetics. At the 2-year posttreatment follow-up, the results were satisfactory. The success of the sagittal relationship correction between the maxilla and the mandible for a skeletal Class III malocclusion depends on the coordination of transverse and vertical relationships combined with the growth potential of each patient.
The treatment for a skeletal Class III malocclusion with an open bite is among the most challenging. These patients have vertical facial growth patterns that manifest clinically as length disharmonies between the maxilla and the mandible in the sagittal plane. Clockwise rotation occurs with the growth and development of the mandible in patients with bad tongue habits, which not only increase treatment difficulty but also increase the possibility of recurrence.
Patients with a skeletal Class III malocclusion are often advised to wait until adulthood for combined orthodontic and orthognathic surgery, but the potential risks and expenses involved are not acceptable to all patients. Since its introduction in the 1960s, facemask therapy has made it possible to direct and stimulate maxillary protraction growth with extraoral force. Several studies have shown that the position and the dimensions of the dentofacial complex can be effectively changed with a facemask or a maxillary expansion appliance in the early period of growth and development of patients with a skeletal Class III malocclusion. Because of molar extrusion and the horizontal force exerted by the chincap, mandibular clockwise rotation is a typical result of facemask or maxillary expansion treatment. Therefore, facemask therapy is more suitable for patients with a skeletal Class III malocclusion and a horizontal growth pattern.
The growth pattern of the maxillofacial region is set after birth, and it rarely changes in a person’s lifetime. In patients unwilling to undergo surgery, interference with the direction and quantity of jaw growth during the early growth period is the sole option. This can help to establish a favorable maxillofacial structure. To some extent, the selection and success of treatment relies on the growth potential of each patient with a skeletal Class III malocclusion.
In this case report, we present the treatment of an 8-year-old girl; her parents were unwilling to have her undergo surgical treatment for her skeletal Class III malocclusion. Instead, she was treated with a facemask, maxillary expansion, and a molar occlusal splint for stimulation of maxillary development and control of vertical jaw growth. After the orthopedic therapy, 2 × 4 technology was used to adjust the molar positions. This case report highlights a treatment that used the patient’s physiologic skeletal, muscular, and dental movements to achieve the desired correction.
Diagnosis and etiology
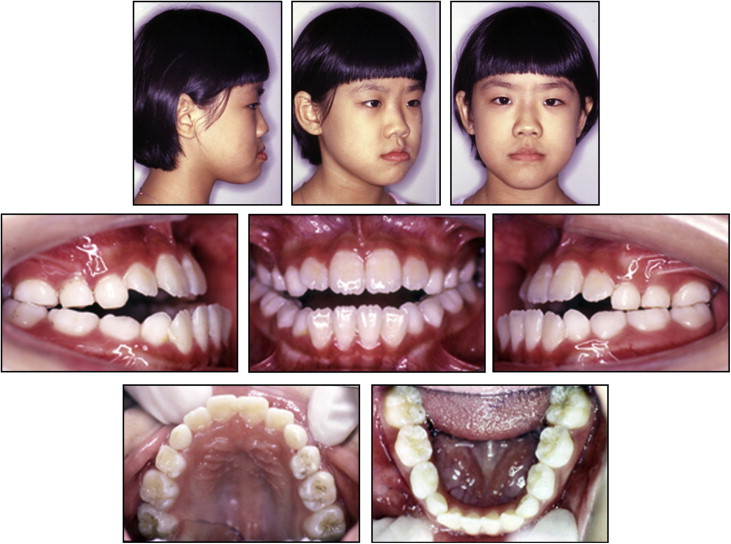
The patient was a girl aged 8 years with no relevant medical history of bone or dental pathology in her family, but she had bad tongue habits. The extraoral examination showed a midface deficiency along with a Class III profile ( Fig 1 ). The intraoral examination showed a Class III malocclusion with posterior and anterior crossbites and with anterior open bite.
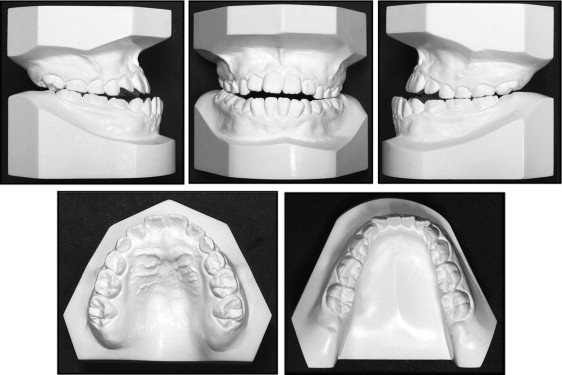
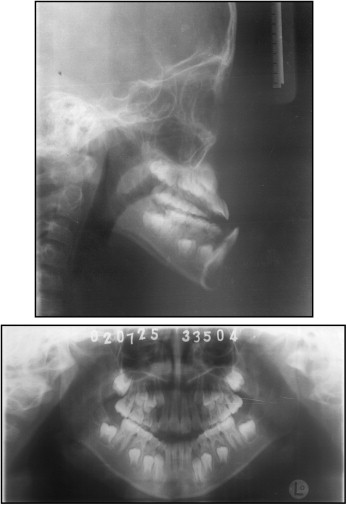
The dental casts ( Fig 2 ) showed a transverse deficiency and an arch length deficiency in the maxillary arch. Moreover, molar and canine Class III relationships coexisted with the anterior and posterior crossbites and the anterior open bite of 3 mm. The panoramic radiograph ( Fig 3 ) showed no hypodontia (and normal periodontal conditions).
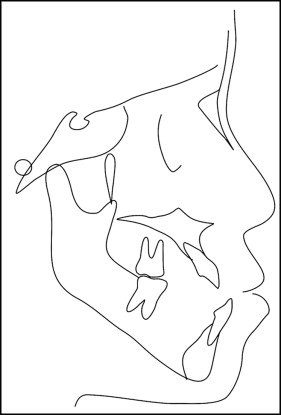
The cephalometric analysis showed a skeletal Class III relationship (ANB angle, −5°) with mandibular excess (SNB angle, 85°). The maxillofacial region had a vertical growth pattern (S-Go/N-Me, 58.8%), but the y-axis angle was basically normal (y-axis, 60°). The mandibular body was long, and the ramus was obviously short (Go-Pg, 79 mm; Go-Co, 48 mm). The position and size of the maxilla were deficient (SNA angle, 80°). The mandibular incisors were lingually inclined (L1-NB angle, 27°). The maxillary incisors were labially inclined (U1-L1 angle, 119°; U1-SN angle, 62°; U1-NA angle, 37°). The eruption of the maxillary incisors and the mandibular molars was deficient (U1-PP, 24 mm; L6-MP, 26 mm) ( Fig 4 , Table ).
| Variable | Mean | A1 | A2 | B |
|---|---|---|---|---|
| SNA (°) | 82 | 80 | 84 | 83 |
| SNB (°) | 79 | 85 | 82 | 81 |
| ANB (°) | 3 | −5 | 2 | 2 |
| U1-L1 (°) | 126 | 119 | 115 | 123 |
| L1-NB (°) | 27 | 27 | 27 | 19 |
| U1-NA (°) | 24 | 37 | 37 | 37 |
| U1-SN (°) | 72.5 | 62 | 59 | 60 |
| PP-FH (°) | 4.5 | −9 | 4 | 1 |
| Y-axis (°) | 61 | 60 | 59 | 60 |
| S-Go/N-Me (%) | 65.8 | 58.8 | 59.7 | 59.3 |
| Go-Co (mm) | 56 | 48 | 55 | 59 |
| Go-Pg (mm) | 72.5 | 79 | 79 | 79 |
| U1-PP (mm) | 27.5 | 24 | 28 | 28 |
| L6-MP (mm) | 33 | 26 | 32 | 32 |
Treatment objectives
The proposed primary treatment objectives were as follows.
- 1.
Stabilize the maxillary and mandibular vertical relationship.
- 2.
Eliminate the functional limitation of the mandible by transverse expansion of the maxillary arch in the early period.
- 3.
Coordinate the maxillary and mandibular sagittal relationships by correction of the dental malocclusion.
- 4.
Obtain a normal posterior overjet and correct the anterior open bite and anterior crowding.
Treatment objectives
The proposed primary treatment objectives were as follows.
- 1.
Stabilize the maxillary and mandibular vertical relationship.
- 2.
Eliminate the functional limitation of the mandible by transverse expansion of the maxillary arch in the early period.
- 3.
Coordinate the maxillary and mandibular sagittal relationships by correction of the dental malocclusion.
- 4.
Obtain a normal posterior overjet and correct the anterior open bite and anterior crowding.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


