and Augusto Ureña1
(1)
Department of Orthodontics, Maimonides University, Buenos Aires, Argentina
The importance of the facts that people place on an esthetically pleasing smile has grown considerably over the last years.
Esthetics is not only important for people as a result of the treatment but during the treatment itself.
Lingual orthodontics is the perfect answer for these patients, since they can achieve the desired results without visible brackets.
This chapter will focus on three of the most frequent types of clinical cases that adults have. The following examples demonstrate three of the most common problems the patients would like treated. The first case was treated with the extraction of the upper first bicuspids in spite of a significant compression of the upper arch. In the second one, the spaces of a previously extracted upper and lower first molars were closed, and in the third clinical case, correction of Class II molar with a pronounced deep overbite was corrected using a combination of pendulum and lingual brackets.
It will provide a step by step description on how to treat them, achieving outstanding results with a very controlled protocol.
These results can be achieved regardless of the type of lingual brackets used. Diagnosis, anchorage, treatment, and retention plan are the most important factors to consider (Harfin and Ureña 2010).
Closing extraction spaces with lingual orthodontics requires making a critical protocol to avoid undesirable tooth inclination or torque.
It is essential to align and level the arches and overcorrect the anterior torque before the retraction process begins.
Since every patient is different, individualized treatment and biomechanics is required.
Case Study 1
This is a 36-year-old patient who complained about upper and lower crowding in combination with upper incisor protrusion. She had no history of general disease or trauma.
Compression of the upper arch, more on the right side, was evident.
Upper and lower midlines weren’t coincident (Fig. 7.1a, b).
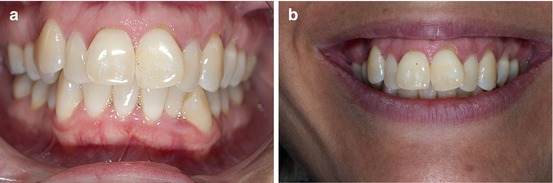
Fig. 7.1
(a, b) Front photographs of a 36-year-old patient with an evident compression on the right side
Class I right and left molar was present. The first upper bicuspids had an observable gingival retraction and the lower left canine was mesioinclined.
Oral hygiene was fairly good (Fig. 7.2a, b).
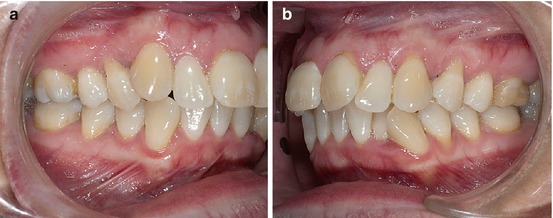
Fig. 7.2
(a, b) Pretreatment lateral views
There was 5 mm of discrepancy in the upper arch and 6 mm in the lower. Some restorations had to be changed and improved. The lateral compression of the lateral sides was clearly visible (Fig. 7.3a, b).
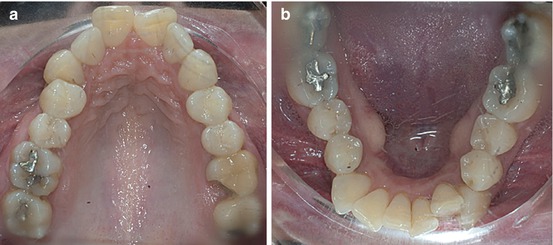
Fig. 7.3
(a, b) Upper and lower arches at the beginning of the treatment
The panoramic radiograph confirmed that the third molars had been extracted during the previous orthodontic treatment and no important bone loss was present.
Cephalometric evaluation revealed the visible proclination of the upper incisors (+11°) and the protrusion of the upper lip (Fig. 7.4a, b).
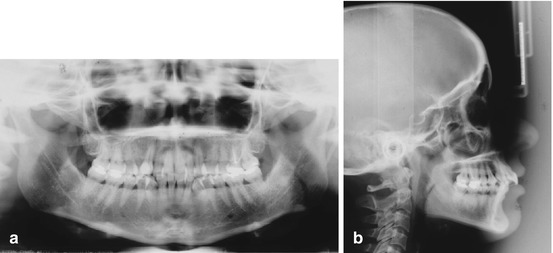
Fig. 7.4
(a, b) Panoramic and lateral radiographs before treatment
Treatments Objectives
1.
Align and level de arches.
2.
Achieve normal overjet and overbite.
3.
Improve smile esthetics.
4.
Maintain periodontal health.
5.
Long-term stability.
Treatment Plan
To achieve the treatment objectives in this nongrowing patient, the extraction of the right and left first bicuspids was recommended.
For personal reasons, esthetic brackets were used on the lower arch with a non-extraction protocol.
A long-term fixed retention plan was suggested.
To initiate the alignment phase, lingual brackets (STB lingual brackets, Ormco Corporation) were bonded indirectly from second molar to second molar except the first upper bicuspids, right cuspid, and left central incisor. A slight open coil spring was added to gain space for the upper central incisor (Fig. 7.5a, b).
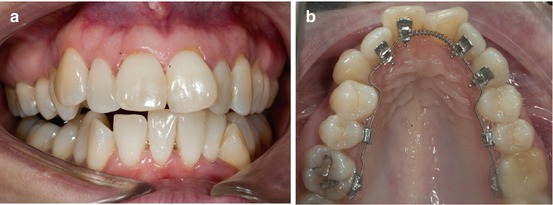
Fig. 7.5
(a, b) Front and occlusal photographs at the beginning of the treatment
After 3 months and when the upper incisors were almost aligned, the extraction of the first bicuspids was performed and a 0.016″ TMA archwire was placed to complete Phase I.
For esthetic reasons, a composite pontic was bonded on the mesial and labial surface of the second bicuspids (Fig. 7.6a, b).
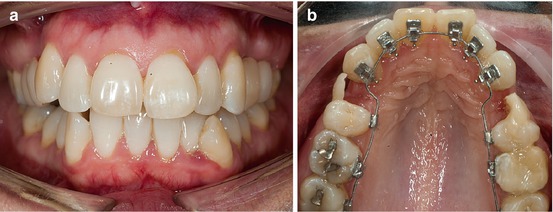
Fig. 7.6
(a, b) After 3 months of treatment with the extraction of the first bicuspids and the esthetic pontics in place
Sliding mechanics was recommended to close the extraction spaces and retrude the upper anterior teeth. A figure-of-eight ligature between the upper canines was recommended to achieve en masse retraction.
To avoid transverse bowing side effect, sagittal and transversal reverse curves were added to the 0.0175″ × 0.0175″ TMA archwire (Fig. 7.7a, b).
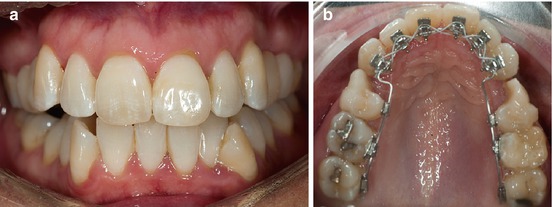
Fig. 7.7
(a, b) Front and occlusal view using sliding mechanics to close the extraction spaces
When nearly 50 % of the extraction spaces were closed, lower esthetic pre-programmed brackets with metal slot were bonded from the first right molar to the left first molar with a stainless steel 0.014″ archwire to begin the alignment and leveling phase (Fig. 7.8a, b).
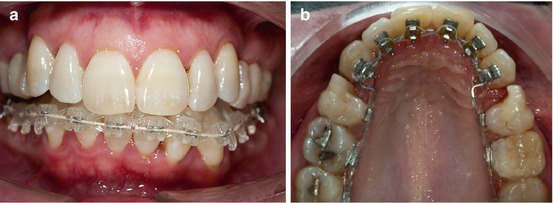
Fig. 7.8
(a, b) After 6 months in treatment, lower esthetic brackets were bonded from the first right molar to the left first molar
A control and pre-programmed mesiodistal enamel reduction were performed in the lower arch to normalize the anterior and canine crowding.
A manual technique using abrasive metallic strips was recommended, especially for the lower anterior teeth, to avoid gingival tissue damage (Fig. 7.9a, b).
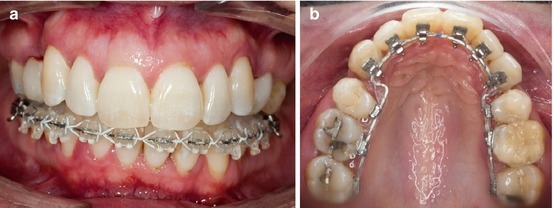
Fig. 7.9
(a, b) Results after a controlled stripping procedure in the lower arch
Before the stripping is performed, it is important to know the thickness of the enamel, the inter-root spaces, and the relation between the width of the root and the shape of the crowns. Six sessions were necessary to complete the correction of the crowded teeth.
For better control, it was advisable that the enamel reduction be performed during several appointments (Fig. 7.10a, b).
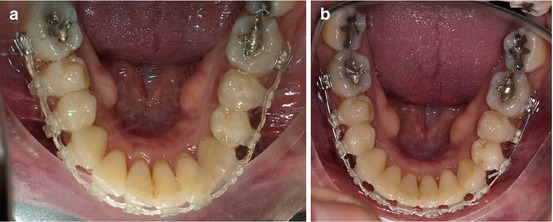
Fig. 7.10
(a, b) The normalization of the incisor and canine position is clearly visible
As always, careful polishing of the stripped areas with composite strips is highly recommended in addition to daily fluoride buccal rinses to enhance remineralization.
These are the results at the end of 22 months of treatment. The treatment objectives were fully achieved. Overjet and overbite were normalized as well as the lower anterior crowding (Fig. 7.11a, b).

Fig. 7.11
(a, b) Final front photographs after 22 months of treatment
All the extraction spaces were closed and Class I right and left canine was achieved. The occlusal plane was almost parallel to the gingival line. No more gingival recessions were observed (Fig. 7.12a, b).

Fig. 7.12
(a, b) Right and left views at the end of the treatment. Class I right and left canine was achieved
For retention, a 0.0195″ multistrand stainless steel lingual fixed retainer was bonded from the right to the left canine in the upper and lower arches (Fig. 7.13a, b).
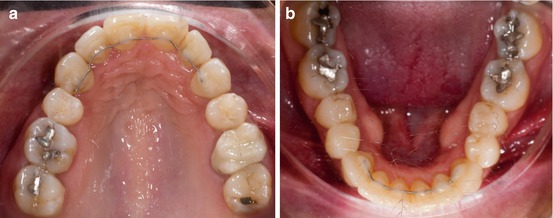
Fig. 7.13
(a, b) Upper and lower arches with fixed retention in place. All the extraction spaces were closed
An upper nightguard was also recommended to reduce dental wear resulting from bruxism.
Smile comparison pre- and post-treatment showed a wider smile despite the fact that the first upper bicuspids had been extracted (Fig. 7.14a, b).

Fig. 7.14
(a, b) Comparison pre- and postsmile photographs
A control 2 years later showed that the smile was improved and normal interdental gingival papillae in the upper and lower arches were achieved (Fig. 7.15a, b).

Fig. 7.15
(a, b) Control 2 years post-treatment
Class I canine and lateral occlusion were maintained along with normal gingivo-periodontal tissues (Fig. 7.16a, b).
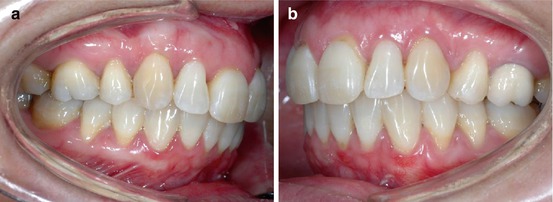
Fig. 7.16
(a, b) Right and left photographs 2 years after treatment
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


