and Augusto Ureña1
(1)
Department of Orthodontics, Maimonides University, Buenos Aires, Argentina
The treatment of impacted canines is a true challenge not only for the orthodontist or the surgeon but for the patients too. Its prevalence is about 1 % in the general population (Warford et al. 2003).
It was described that 85 % of them are palatal impactions and only 15 % are labial impactions (Thilander and Jakobson 1968).
Since the maxillary canines have the longest distance between the place of their formation and the place of eruption, they are more liable to problems in their path of eruption.
They play a vital role in facial appearance, dental esthetics, arch development, and functional occlusion.
The most common reasons that cause impaction are usually localized: lack of space, supernumerary teeth, tumors, dentigerous cysts, trauma, dilacerations of the root, idiopathic conditions, or aberration in the normal pattern of eruption (Bishara 1992, 1998).
Some studies have suggested that peg-shaped or missing lateral incisors could be an etiological factor (Becker et al. 1984; Becker and Chaushu 2003; Brin et al. 1986).
Its early detection may reduce complications and treatment time.
Ideally, the orthodontic treatment of a palatally impacted canine is to bring the tooth to its normal position without causing any periodontal, tissue, or tooth damage.
Where prognosis is a concern, normally it is good. There is a positive correlation between the original position of the canine, root shape and length, type and height of periodontal attachment, and dilacerations of the root. The surgical protocol and type of biomechanics during and after the surgical procedure is important, no matter which type of brackets is used.
Resorption of the central or lateral incisor roots can be expected to be present in 30–40 % of the cases, and they are visualized about 50 % more often by CT scanning than by intraoral X-rays (Ericson and Kurol 1986, 1987a, 2000; Mah and Alexandroni 2010).
Working together with the surgeon is of paramount importance (Cassiano et al. 2012).
Although digital panoramics or periapical Rxs provide satisfactory diagnostic images, they lack the accuracy necessary for assessing buccal or palatal root resorption of the adjacent teeth (Ericson and Kurol 2000).
New diagnostic tools as cone beam and three-dimensional radiographs are fundamental to determine the real position of the impacted canine (Fig. 6.1a, b).
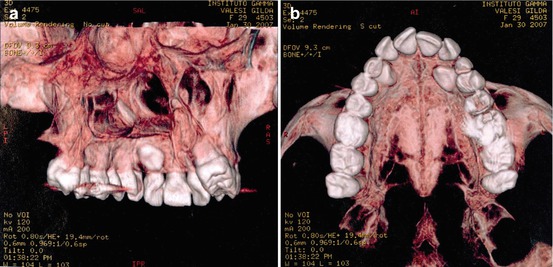
Fig. 6.1
(a, b) Three-dimensional radiographs are relevant to determine the exact position of the impacted canines.
The best surgical treatment has to be determined by the surgeon, according to its tridimensional position, amount of bone, etc.
It is highly recommended that the surgical exposure and placement of a bracket or an auxiliary attachment be performed in the same procedure (Chaushu et al. 2004).
There are some cases where extraction would be the best choice specially when there is no space between the lateral incisor and the bicuspid and the canine is displaced too high. Extraction is also indicated when the tooth is ankylosed or with an evident dilacerated root. Another situation could be when the canine is lodged between the roots of the central incisors or between the roots of the central and lateral incisors and orthodontic movement would jeopardize these teeth (Becker 1981, 2010).
Creating adequate space in the dental arch to accommodate the impacted canine before the surgical procedure is suggested.
A new lingual ballista spring was developed by the authors to improve the eruption of impacted canines (Fig. 6.2a).
It is easy to make and manipulate. TMA 0.0175″ × 0.0175″ wire or 0.018″ SS is recommendable to make the ballista spring.
The design includes a distal and a mesial loop for better force and torque control. The distal one is located in front of the molar tube and the mesial one on the palatal side of the first bicuspid. The activation is done by a wire ligature (Fig. 6.2b) every 3–4 weeks.
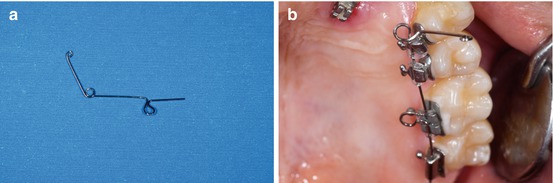
Fig. 6.2
(a, b) New lingual ballista spring and its activation
It is very simple to construct, insert, and ligate as it is independent from other parts of the appliance.
The force of the spring is proportional to the diameter and length of the wire and allows the extrusion of the canine without compressing the canine toward the adjacent teeth. The force is well controlled and easily modified according to the original position of the impacted tooth (Fig. 6.3a, b).
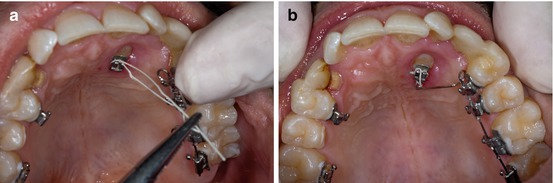
Fig. 6.3
(a, b) Activation and ligation of the ballista spring
It is strongly recommended that the tooth be erupted vertically and downward through the palatal tissue and then moved buccally into its place in the arch.
Another option is to use the ballista spring to erupt the canine before the anterior brackets are placed.
This protocol helps protect the roots of the adjacent teeth.
The canine should be moved using light and continuous force, not exceeding 80–100 gs.
A controlled anchorage is necessary to avoid unwanted effects on the molars or anchorage unit.
This 28-year-old patient came to the office looking for an esthetic solution.
She had lost the temporary canine 1 week earlier and was worried about it (Fig. 6.4a, b).
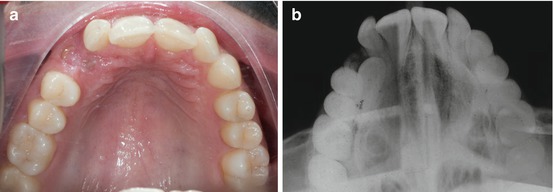
Fig. 6.4
(a, b) Occlusal photograph and radiograph of a 28-year-old patient with an impacted right canine
The occlusal Rx showed the position of the canine and the length of the root. The objective of the treatment was to proper position the impacted upper right canine into the arch.
One week after the surgery, the traction phase began.
It is highly advisable to move the impacted canine occlusally first, and when the whole crown is totally erupted, a buccal movement can begin.
If the canine is in close proximity to the incisor roots and a buccally directed and heavy force is applied, it will contact the roots and may cause important and irreversible damage to them.
Composite temporary crown was placed in order to improve esthetics. It is recommendable for temporary composite pontics to be bonded on the labial and mesial surface of the first bicuspid (Fig. 6.5a).
After the crown of the canine was totally erupted, an open coil spring was used to gain space for the upper lateral incisors in combination with a 0.016″ TMA arch (Fig. 6.5b).
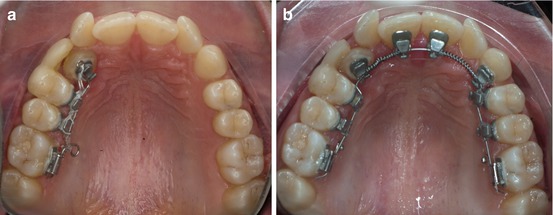
Fig. 6.5
(a, b) Occlusal view with the temporary crown in place and with the open coil spring to gain space for the lateral incisors
Three months later, the upper lateral incisors were bonded (Fig. 6.6a, b) to complete the upper arch.
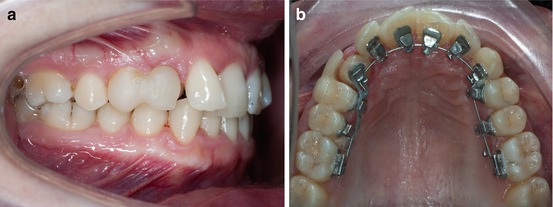
Fig. 6.6
(a, b) Brackets on the upper lateral incisors were bonded with individual caps
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


