Fig. 6.1
The MTA mix. Note the consistency of the paste
6.2.2 Insertion
The MTA should be inserted in place immediately after handling, avoiding its dehydration. A Lentulo spiral can be used for its insertion or alternatively a micro amalgam carrier, gutta-percha plugger, Map system, Dovgan applicator, or ultrasound (Fig. 6.2).
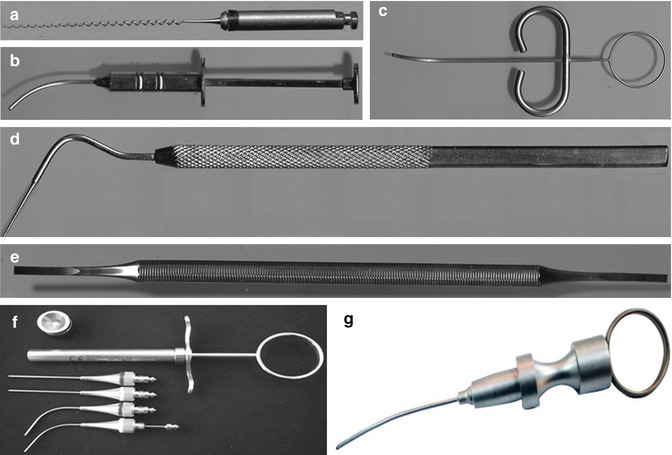
Fig. 6.2
Insertion devices for MTA: (a) Lentulo spiral, (b) amalgam micro-carrier, (c) MTA carrier, (d) gutta-percha plugger, (e) chisel, (f) Map system, and (g) Dovgan applicator
6.3 Clinical Applications of MTA
The variety of MTA uses include:
(a)
Direct or indirect pulp capping
(b)
Pulpotomy
(c)
Incomplete root formation
(d)
Perforation
(e)
Canal obturation
(f)
Endodontic surgery
(g)
Internal or external tooth resorption
(h)
Root fracture
(i)
Revascularization
6.3.1 Direct Pulp Capping
Direct pulp capping is performed when there is accidental exposure of the pulp, with the goal of maintaining pulp vitality and facilitating the formation of mineralized tissue, thus sealing the exposure.
MTA used for direct pulp capping has exhibited a similar or superior response to calcium hydroxide, leading to formation of a mineralized barrier, in addition to its sealing ability [1, 2, 21, 28, 41, 43, 48, 58, 71, 75, 83]. In one study [58], 69 direct pulp protections performed with MTA and 53 with calcium hydroxide were assessed, and a higher success rate was demonstrated with MTA.
After confirmation of the exposure of the pulp tissue and the conditions thereof, the cavity is irrigated with saline solution to remove dentinal pulp waste and achieve pulp hemostasis. The MTA should be applied with care so as to not compress the material into the pulp cavity. All material that is on the surrounding walls should be removed with a curette and the cavity sealed with a restorative material (Fig. 6.3).
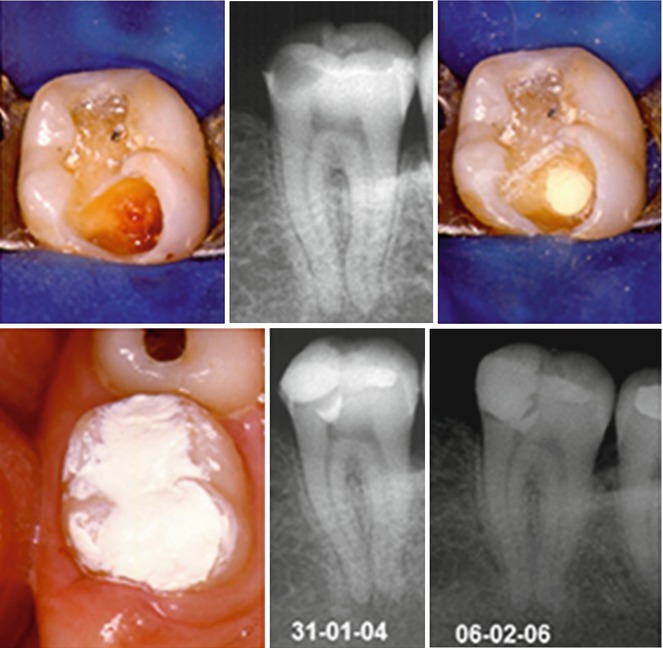
Fig. 6.3
Direct pulp capping with MTA
6.3.2 Pulpotomy
Pulpotomy involves the removal of the coronal pulp, maintaining the radicular, and is indicated when there is irreversible inflammation of the coronal pulp, and particularly indicated in the teeth with incomplete root formation.
In a histological study [41] where pulpotomy procedures were performed on dog teeth, a better dentine bridge formation occurred with cases treated with MTA than in those where calcium hydroxide was employed. Other authors also confirmed the efficiency of the MTA in the pulpotomy procedure [11, 15, 41, 56, 74].
After the coronal opening, the coronal pulp is removed with a curette, followed by irrigation with saline solution. The MTA is placed over the pulp tissue without pressure, at a thickness of approximately 3 mm. Calcium hydroxide paste can be placed over it, consistently well, and the cavity closed with a restorative material (Fig. 6.4). The calcium hydroxide paste is placed over the MTA in order to avoid direct contact of the sealant with the MTA, especially when the restoration is performed in the same session.
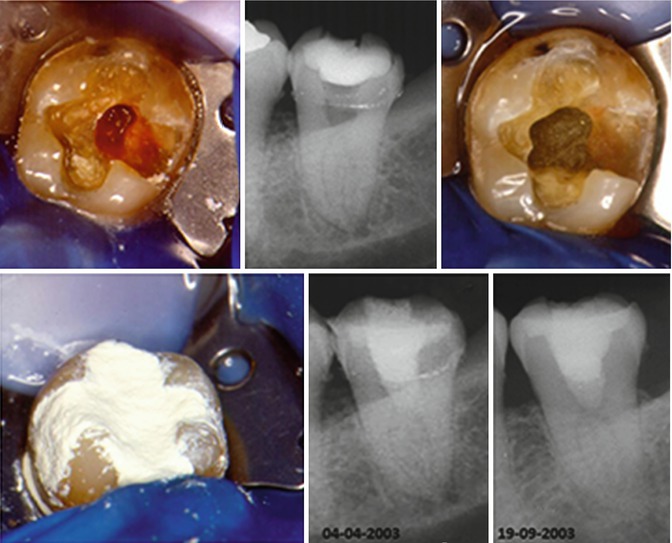
Fig. 6.4
Pulpotomy with MTA
The repair occurs by the formation of a mineralized tissue on the remaining radicular pulp (Fig. 6.5).
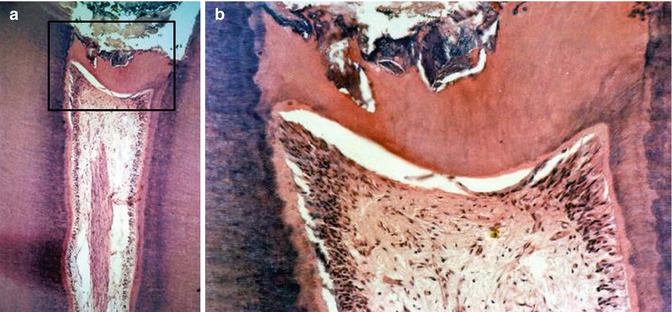
Fig. 6.5
(a) Mineralized tissue formed after pulpotomy with MTA; (b) largest increase in the marked area
6.3.3 Incomplete Root Formation
The tooth with incomplete root formation constitutes a problem for endodontic treatment. Because the apex is not completely formed, there is difficulty in instrumentation and obturation of the canal, and there is a great risk of extrusion of material from the apical region. Apexification is defined as a method to induce formation of the mineralized barrier on the open root apex or the continued apex development of the tooth. Calcium hydroxide has been the material of choice for this procedure with periodic changes lasting from 5 to 20 months in order to induce the formation of the mineralized barrier. The process is slow with vulnerability to the temporary sealing, with a possible occurrence of recontamination, tooth fracture, and an unpredictable outcome [5, 6, 69]. For these reasons, apexification in one or two sessions using MTA has been proposed [61, 62], with the goal of a more rapid completion of the case.
After instrumentation of the canal, the MTA is placed in small portions in the apical region with the aid of a Lentulo spiral. The Map system or Dovgan applicator is used to obtain the apical plug which must be 3–5 mm (ideally 5 mm). With a K file or Hedstrom file wrapped in cotton compatible with the canal size, the vertical compaction of the MTA is performed. Alternatively, the compaction can be performed with a gutta-percha plugger. The radiograph is taken to confirm the presence of the apical plug, and if it is not satisfactory, the MTA is removed by irrigation with saline solution and the procedure is repeated. The canal obturation follows with gutta-percha and sealer. If the obturation is not performed in the same session, the canal can be filled with a slurry of calcium hydroxide dressing which remains as a temporary dressing for a maximum of 30 days (Fig. 6.6).
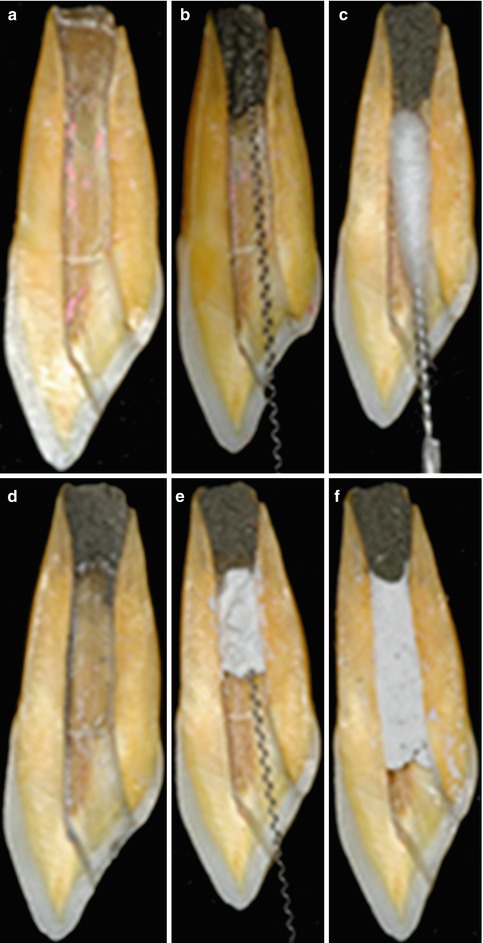
Fig. 6.6
Fabricating the apical plug with the aid of a Lentulo spiral and endodontic file. (a) Tooth with incomplete apices; (b) Insertion of MTA; (c) Compactation of MTA; (d) Tooth with MTA in the apical portion; (e) Filling the other canal portions with callcium hydroxide; (f) Tooth with the canal filled with MTA and calcium hydroxide paste
A success rate of 90 % was observed when the MTA apical plug was placed via the canal [59, 61]. Other studies have also observed a complete root formation in the teeth with open apices treated with MTA [4, 24, 25, 27, 30, 35, 38, 44, 49, 55, 61, 63, 77, 78].
The apical plug can also be placed by completely filling the canal with MTA to then immediately removing it to the desired length with a K file, leaving only the part corresponding to the apical plug. Next, with a K file wrapped in cotton, the MTA is compacted (Fig. 6.7). All the material that is on the walls of the canal should be removed in the same session that the MTA is inserted in the canal as after it sets MTA is difficult and sometimes impossible to remove. The apical plug should ideally be 5 mm [84] and may be greater depending on the foramen opening of the root.
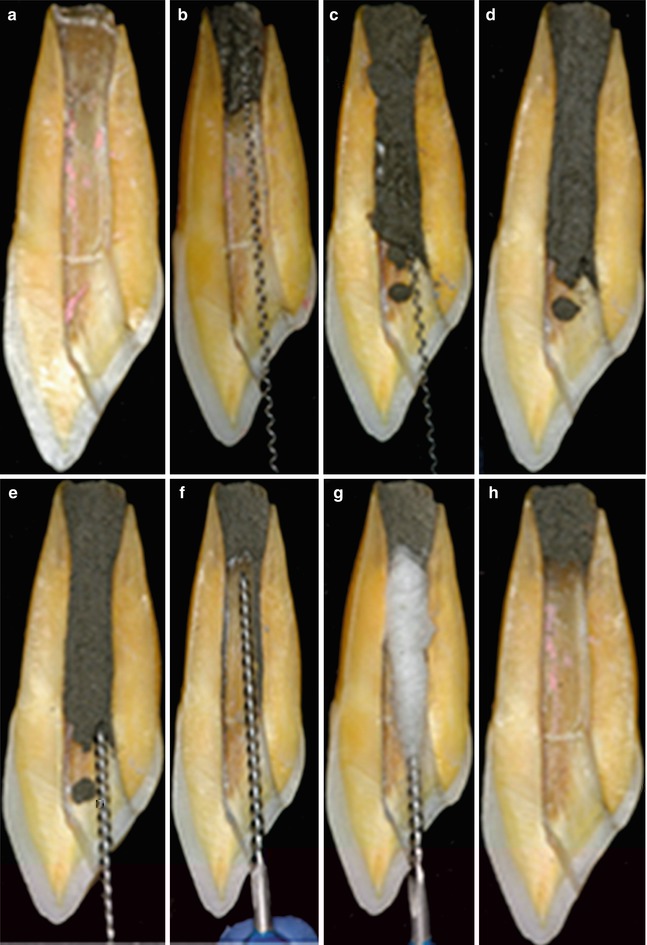
Fig. 6.7
Fabricating the apical “plug” by filling the entire canal with MTA and then adjusting the desired length with a file. (a–d) Sequence of entire root canal filled with MTA; (e–g) remotion of the MTA in the cervical and medium portion of the canal; (h) Tooth with the apical portion filled with MTA
If the apical plug provides adequate resistance, the obturation of the canal could be done in the same session; otherwise the remainder of the canal should be filled with calcium hydroxide paste, leaving the obturation to be completed in successive treatment session when the MTA setting is complete (Figs. 6.8 and 6.9).
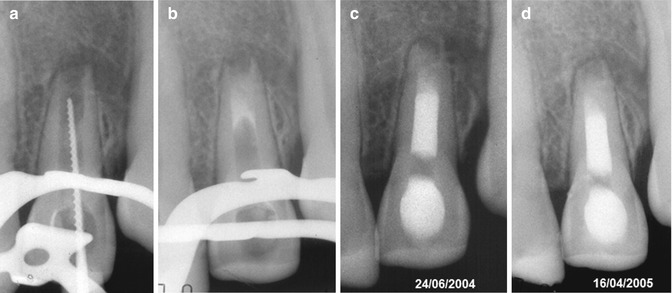
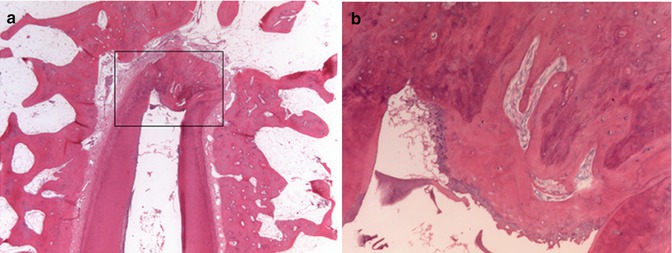
Fig. 6.8
The MTA apical plug in the treatment of the teeth with incomplete root formation
Fig. 6.9
(a) Mineralized tissue formed at the apex of a tooth with incomplete root formation, treated with MTA; (b) largest increase in the marked area
If the foraminal opening is too wide, extrusion of the MTA from the periapical region can occur, which is not recommended [19, 34, 39, 59, 65]. Placement of a matrix (barrier) of calcium hydroxide, calcium sulfate, or collagen to minimize the extrusion of material into the periapical tissues has been recommended [19, 34]. The extra root matrix (barrier), aside from preventing extrusion of the MTA, prevents contact with tissue fluids or blood during its insertion (Fig. 6.10). These materials are easy to use, are well tolerated by the periodontal tissues, provide a dry field against which the MTA will condensate, and are reabsorbed in a few days, without interfering with the repair process in the region.

Fig. 6.10
Materials used for extra root matrix (barrier): (a) calcium hydroxide, (b) calcium sulfate, and (c) hemostatic collagen
After instrumentation of the canal, the matrix material is brought to the apical region via the canal using a gutta-percha plugger compatible with the diameter of the canal. After the insertion of the apical matrix, the MTA is introduced in the canal with the aid of a Lentulo spiral, Map system, or Dovgan applicator obtaining the apical plug. A root canal filling composed of gutta-percha and sealer completes the final obturation (Figs. 6.11 and 6.12).
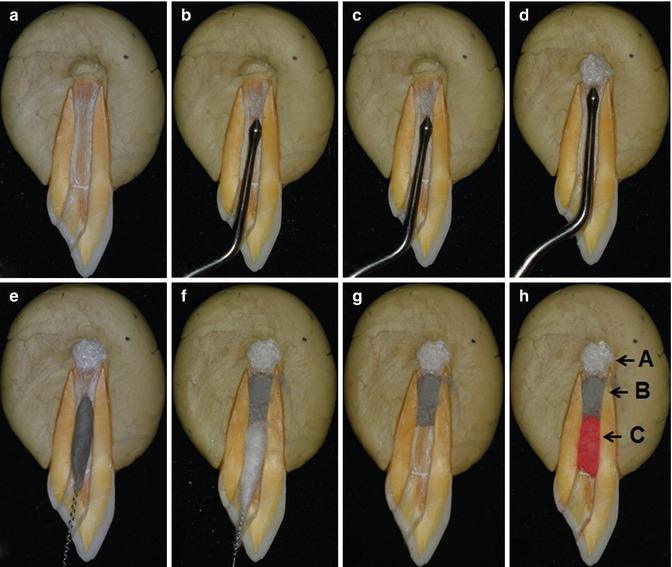
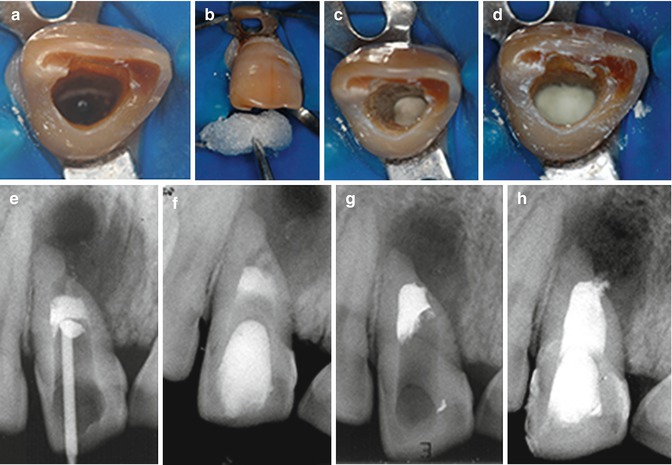
Fig. 6.11
Fabrication of the extra root apical matrix (barrier) with collagen: (A) matrix, (B) MTA, and (C) canal obturation. (a–d) Insertion of the collagen matrix in the periapical tissue; (e–h) Insertion of the MTA in the apical portion and obturation of the remaining portion of the canal
Fig. 6.12
Fabrication of the apical collagen matrix for placement of MTA in the teeth with incomplete root formation
6.3.4 Root Perforation
Root perforation is a common accident occurring during endodontic treatment, resulting in a communication between the pulp cavity and the periodontium and can occur at any stage of treatment and can be located at the level of the pulp chamber and root canal.
The repair of the root perforation occurs with the formation of a mineralized tissue sealing itself, the neoformation of bone tissue, and periodontal ligament reinsertion (Fig. 6.13)
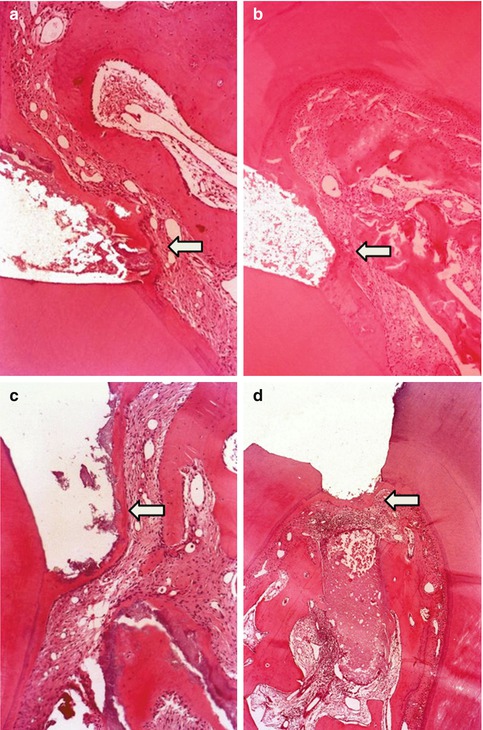
Fig. 6.13
Microscopic aspects of the repair of root perforations treated with MTA (white arrow)
Root perforations have classically been treated using calcium hydroxide, but the large perforations did not respond well to this treatment. With the introduction of MTA, this treatment has become easier and faster, and with predictable results even in large perforations [3, 8, 10, 20, 31, 36–38, 40, 47, 52, 54, 57, 60, 76, 87].
The successful treatment of a root perforation depends on factors such as level, location, size, and presence or absence of contamination. The root perforation treatment with MTA or with calcium hydroxide is indicated in the intra-osseous perforations.
When the root perforation occurs, the sooner the treatment is carried out, the greater is the likelihood of success. The root perforation at the level of the pulp chamber is irrigated with saline solution to clean and control bleeding in order to apply the MTA. A sufficient amount of material is required to seal the root perforation with the gutta-percha plugger. If the tooth is exposed and the root perforation is contaminated, it is important to insert an antiseptic medication before sealing the tooth; in the second session, the medication is removed, and the chamber is irrigated by inserting a calcium hydroxide paste in the root perforation, followed by inserting MTA in the third session.
If the root perforation is intra-canal, after instrumentation, it is filled with calcium hydroxide paste. In the second session, the calcium hydroxide is removed from the canal, hence proceeding with obturation. The obturation is immediately cut to expose the root perforation, proceeding with the sealing with MTA (Fig. 6.14).
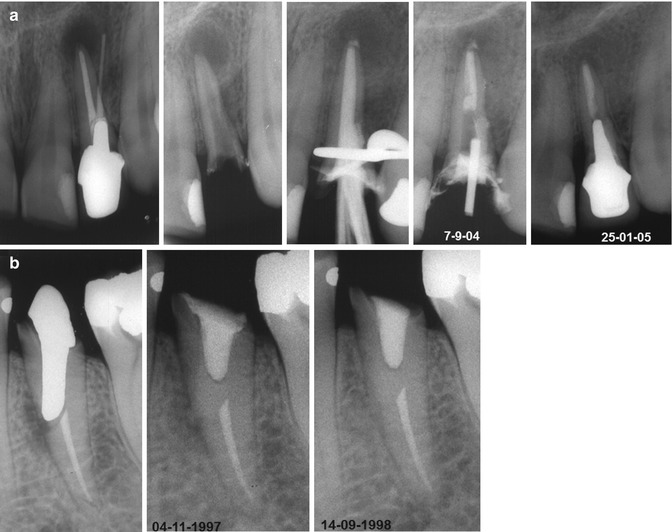
Fig. 6.14
Root perforations sealed with MTA: (a) upper lateral incisor; (b) lower premolar. Observe the repaired area
Extrusion of the MTA may occur if the root perforation is too large, hindering its resorption and repair area. In this case, it is convenient to make use of the extra root barrier with calcium hydroxide, calcium sulfate, and collagen, which must be placed, via the root perforation in the bone cavity ahead of the MTA. The excess barrier material is removed from the path of the root perforation with a K file, compatible with the diameter of the root perforation, followed by insertion of MTA (Figs. 6.15 and 6.16). The importance of the use of the matrix was highlighted by some authors [3, 10, 20, 39, 47, 76].
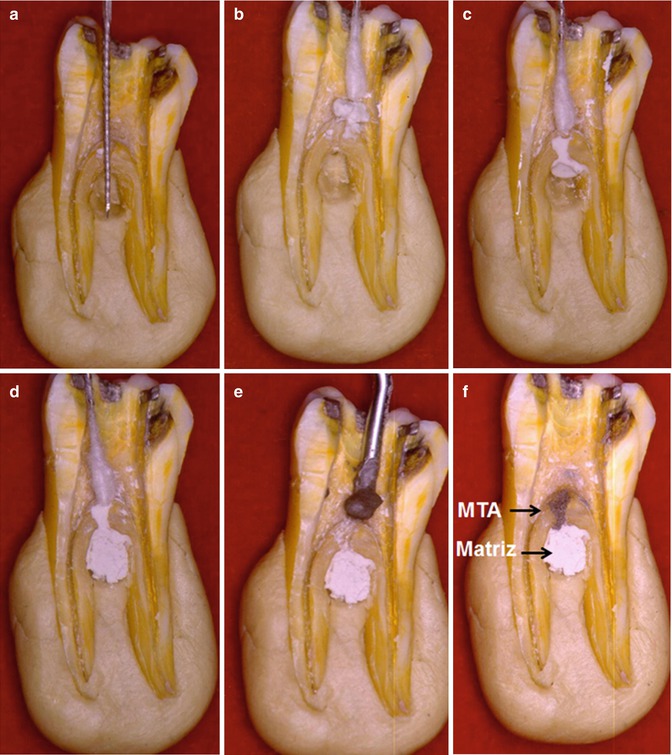
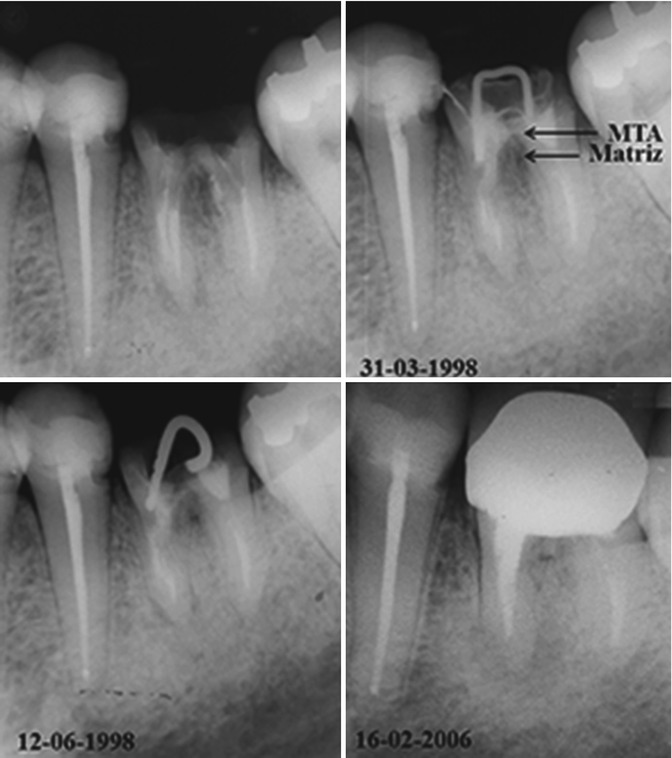
Fig. 6.15
Fabrication of the calcium sulfate matrix and MTA in the root perforation. (a–c) Confection of the matrix with calcium sulphate in the furcal region; (d–f) Insertion of MTA in the furcal perforation
Fig. 6.16
Root perforation treatment with the calcium sulfate matrix and MTA
6.3.5 Canal Obturation
During the root canal preparation, over-instrumentation can occur which may favor the occurrence of over-obturation. In this situation, MTA can be used as an apical plug, with a similar way to the method described for the tooth with incomplete root formation. The larger the size of the instrument past the apex, the greater should be the thickness of the apical plug [23].
After the canal preparation, the apical plug is fabricated with the MTA, inserting it only in the apical region or alternatively completely filling the root canal with the MTA, to then remove part of it, leaving only the portion corresponding to the apical plug (Fig. 6.17), which must be at least 3 mm thick [4, 23, 51, 69].
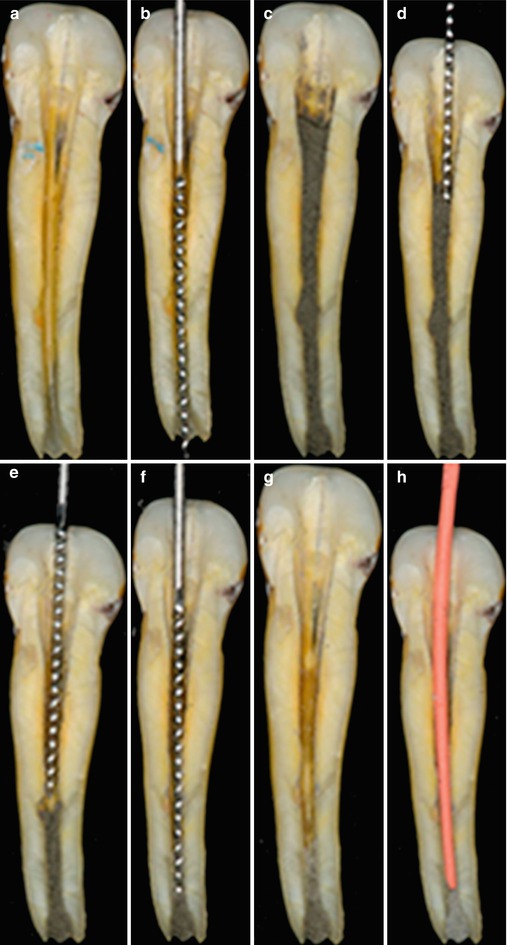
Fig. 6.17
Fabrication of the apical plug with MTA in an over-instrumented canal. (a–d) Root canal preparation and obturation wth MTA; (e–h) Remotion of MTA in the cervical and medium portions of the root canal and insertion of a gutta-percha cone
The root canal filling can be done in the same session or on a consecutive visit, depending on the consistency and strength of the apical plug. During the obturation, the cone should be well adjusted to the canal, so as not to exert strong pressure on the apical plug during the obturation, leading to leakage of the material (Fig. 6.18).
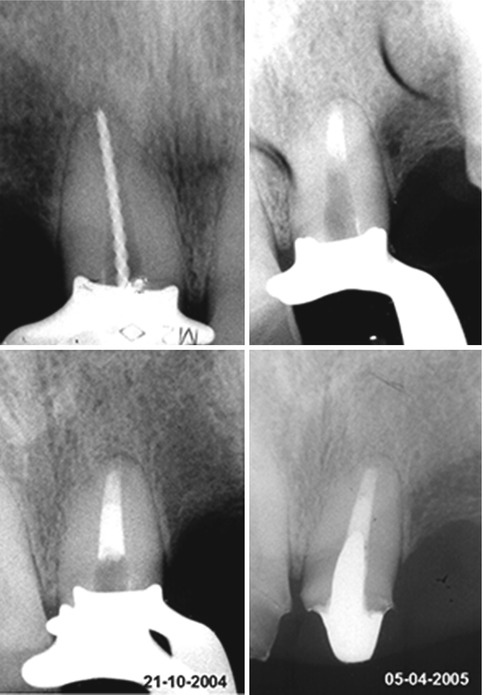
Fig. 6.18
Apical plug with MTA and obturation of the canal with gutta-percha and sealer
6.3.6 Endodontic Surgery
When endodontic treatment fails or retreatment is not possible, endodontic surgery is indicated. Among the different types of surgery is the retrograde filling, which consists of the preparation of an apical cavity and its filling with retro-obturation material. The MTA is highly indicated for retrograde filling [7, 9, 13, 16, 22, 26, 51, 72, 79–82].
The retro apical cavity is prepared with ultrasound, trying to follow the direction of the canal, with a depth of 3–5 mm, maintaining retention and regularity. The MTA should have a consistency that facilitates its insertion into the cavity by means of a Lucas curette, Map system, or Dovgan applicator.
After placement of the MTA, the surgical wound should not be irrigated, since this can result in dislodgement of the material from the retro-cavity. Excess material should be removed with Gracey or Lucas curettes or gauze moistened with saline solution (Fig. 6.19).
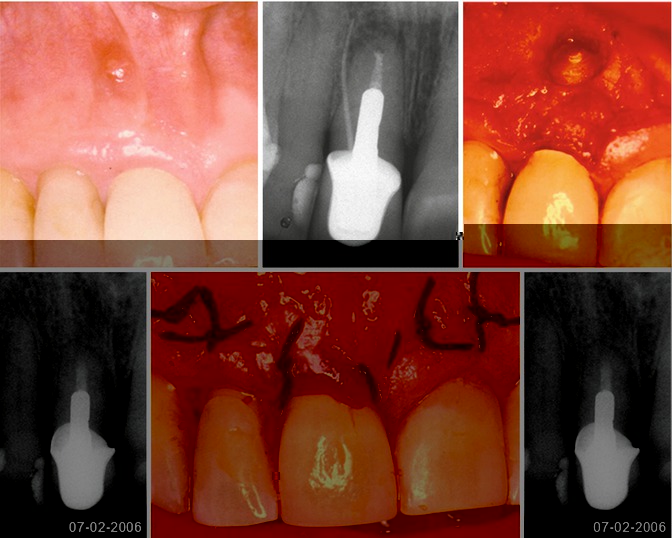
Fig. 6.19
Retrograde filling in the maxillary central incisor with the use of MTA
6.3.7 Tooth Resorption
External or internal tooth resorption is a multifactorial pathology and may be caused by pulp necrosis, dental trauma, orthodontic tooth movement, tooth whitening, and more. The internal and external resorption can cause communication of the canal with the periodontium, and in this case, the treatment is more difficult with a doubtful prognosis.
The resorption has classically been treated with calcium hydroxide, and more recently with MTA [45, 68]. If the internal resorption is perforated and there is invaginated tissue, it is removed with a K file with its tip bent, followed by irrigation with sodium hypochlorite solution. It is important to use a dressing with calcium hydroxide, until all the invaginated tissue is totally eliminated. The MTA is delivered to the canal with a Lentulo spiral, Map system, or Dovgan applicator, filling the entire area of resorption (Fig. 6.20).

Fig. 6.20
Apical resorption treated with MTA
6.3.8 Root Fractures
Dental fractures with a traumatic etiology can occur in the crown, root, or crown/root. When in the root, it can be vertical or transversal, and the vertical fracture presents a very poor prognosis. The transversal, depending on their location (cervical, middle, and apical), can have a success outcome in the treatment. The root fracture located in the cervical and middle thirds causes difficulty for treatment because it is difficult for dental immobilization, leading to injury or even preventing the consolidation of the fragments. For these cases, it is possible to strengthen the tooth with an intra-canal pin cemented with MTA [18].
The canal is instrumented, and then an apical plug with MTA is performed. A metal pin is selected in order to remain adjusted in the canal, which is filled with MTA, seating the pin inside. Thus, there is reinforcement for the root, preventing mobility of the coronary segment (Fig. 6.21).
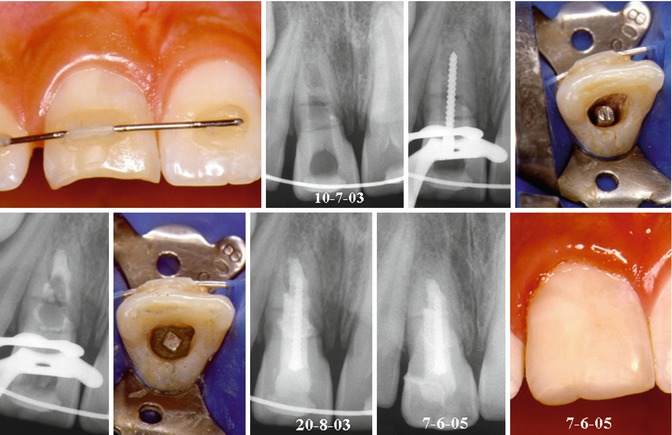
Fig. 6.21
Treatment of root fracture with MTA, reinforced with an intra-canal pin
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


