http://evolve.elsevier.com/Haveles/pharmacology
Antineoplastic agents were designed to treat malignancies. A relatively new use of these agents is in the management of diseases with an inflammatory component such as psoriasis, rheumatoid arthritis, and systemic lupus erythematosus. Depending on their use, these agents are prescribed by oncologists, rheumatologists, or oral pathologists (for oral conditions related to systemic autoimmune diseases). For patients taking these agents to treat malignancies, the dental hygienist should be aware of the relationship between the timing of the treatments and the effects on the bone marrow. The dental hygienist should be familiar with the side effects of these agents, especially their oral manifestations.
Current research is elucidating many different mechanisms involved in the etiology of cancer, including genetics, viruses, deleted or damaged tumor-suppressor genes, specific oncogenes, and changes in both ribonucleic acid (RNA) and deoxyribonucleic acid (DNA) that affect the growth of cells. Many animal carcinogens have been identified, but proving carcinogenic potential in humans is much more difficult.
Many human carcinogens are environmental carcinogens, for example, polychlorinated biphenyls (PCBs) from transformers. Other known carcinogens are tobacco smoke, aflatoxins (produced by moldy peanuts), sunlight (increase in malignant melanoma and squamous cell carcinoma), radiation, chemicals, dioxin, and benzene. Most authorities believe that the herpes viruses and papillomaviruses have a potential for producing cancerous changes. Patients with a history of certain diseases, such as hepatitis, have a higher incidence of liver cancer than patients without such history.
Normal cells have a mechanism to turn off cell growth with certain signals. In cancer, however, a change in the cells occurs so that they continue to grow. With a lack of control (switch does not turn off), the abnormal neoplastic cells continue to grow. The cell-surface antigens appear similar to the normal fetal types, so the body does not mount an immune response. The tumor stem cells have chromosomal abnormalities, repetitions, and select subclones. With repeated cycles, the cells can migrate or metastasize to distant sites, thereby spreading the cancer. For example, cancer that begins in the breast may spread to the bone or liver.
Use of antineoplastic agents
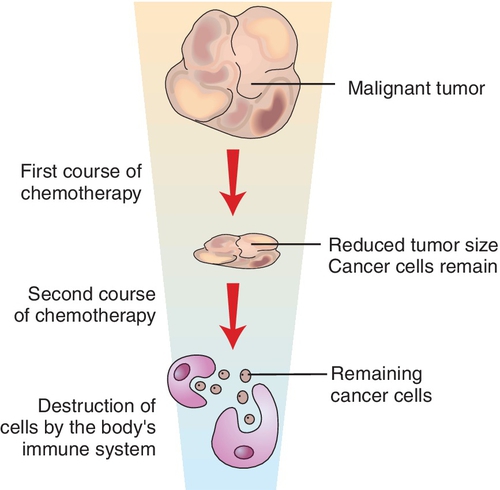
Antineoplastic agents, sometimes called cancer chemotherapeutic agents, are used clinically to interfere with the neoplastic cells. The antineoplastic agents interfere with some function of the malignant cells. They suppress the growth of the cells and attempt to destroy and prevent the spread of malignant cells. (Figure 23-1 illustrates the way in which cancer cells respond to chemotherapy.) These agents are used either alone or in combination or with irradiation or surgery, depending on the type of malignancy being treated. Each type of malignancy may be sensitive to each of the three modalities: drugs, irradiation, or surgery.
For treatment of certain malignancies, for example, the leukemias, choriocarcinoma, multiple myeloma, and Burkitt’s lymphoma, drugs are considered the primary choice. Often, combinations of several antineoplastic agents, used in conjunction with surgery and/or irradiation, may effect a cure that each procedure alone could not. Certain cancers are relatively insensitive to antineoplastic agents. These cancers are treated with either irradiation and/or surgery. Box 23-1 lists malignancies and their likelihood of sensitivity to cancer chemotherapy agents.
The current philosophy for the use of the antineoplastic agents involves treating the initial stages of disease very aggressively. This approach promises more chance of controlling and curing the disease but also involves many severe side effects, including some that affect the oral cavity. The treatment of some cancers involves the removal of cells from the bone marrow before administration of the chemotherapy or irradiation. In the past, the dose administered would have been fatal. However, after treatment is complete, the cells taken from the bone marrow are returned to the patient’s body, and they begin making the blood elements that are made in bone marrow. Gene therapy is being used, and many advances are continuing to be made. New research is attempting to use the body’s immune system to fight the cancer cells.
Mechanisms of action
The efficacy of antineoplastic agents is based primarily on their ability to interfere with the metabolism or reproductive cycle of the tumor cells, thereby destroying them. The reproductive cycle of a cell consists of the following four stages (Figure 23-2):
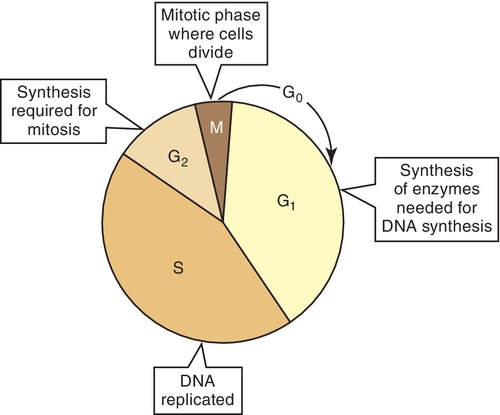
Cells in a resting stage that are not in a process of cell division are described as being in the G0 stage. Cells enter the cycle from the G0 stage. In some tumors, a large proportion of the cells may be at the G0 level. These cells are difficult to reach and destroy.
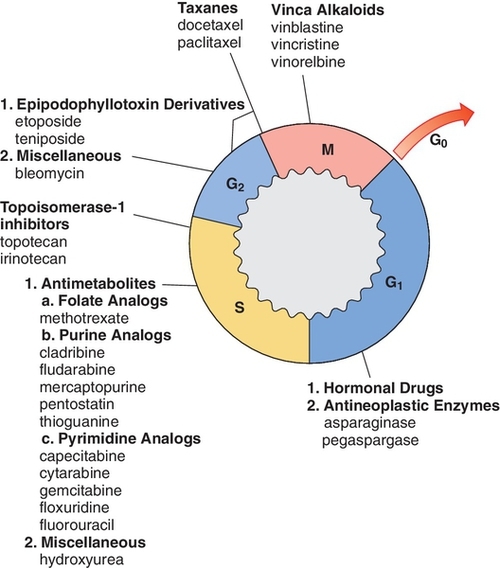
Most of the antineoplastic agents are labeled as being either cell cycle–specific (Table 23-1 and Figure 23-3), indicating that they are effective only at specific phases of cellular growth, or cell cycle–nonspecific, indicating that they are effective at all levels of the cycle (effective both in the resting and the proliferating cells). For example, the alkylating agents interfere with the malignant cells during all phases of the reproductive cycle and the resting stage (G0) and therefore are classified as cycle independent.
Table 23-1
Classification of Antineoplastic Drugs
| Cell cycle—specific | Antimetabolites Bleomycin Vinca alkaloids Podophyllin |
| Cell cycle—nonspecific | Alkylating agents Antibiotics Cisplatin Nitrosoureas |
A major problem with treating neoplastic cells is that the cell growth is exponential. Before diagnosis is made, a large cell load must be present. If 1012 cells are present and 99.9% of the cells are killed, 109 cells would remain; if 99.9% of those cells were killed, 106 cells would still be present. Mixing several chemotherapeutic agents can increase the chance of killing more cells because they work by different mechanisms and have different adverse reactions.
Resistance to chemotherapy occurs by either of the following methods:
Classification
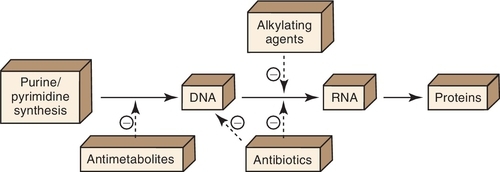
The antineoplastic agents are divided into groups depending on their mechanisms and sites of action (Figure 23-4). Box 23-2 lists some antineoplastic agents by classification.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


