9
Problems with Retainers and Trouble-shooting
The previous chapters on retainers and retention have discussed why retainers are needed; the different types of retainer; how they are checked and fitted; and what needs to be checked at follow-up. We now discuss what can happen during the the long-term follow-up of retainers; what can go wrong and what – if anything – can be done to deal with these problems.
- Explain the main problems associated with retention and retainers
- Advise patients how to manage problems with retainers
- Explain to patients what, realistically, they may expect from orthodontic treatment during and following retention
- Explain to patients why retention may need to be terminated
Problems with Removable Retainers and Trouble-Shooting
The problems that can arise with removable retainers can be grouped in a variety of ways. However, a convenient, but also clinically realistic, way of classifying the problems is as follows:
- Problems the patient is aware of
- Problems the patient is unlikely to be aware of.
All the problems that can arise, either directly or indirectly, ultimately affect whether or not alignment can be maintained, and to what extent some level of misalignment has to be accepted. Furthermore, in the UK at least, in many clinical settings, the patient may also incur charges, e.g. for the replacement or repair of retainers.
Problems the Patient Is Aware Of
- Lack of fit
- Lack of alignment
- Discomfort
- Lack of patient motivation
- Breakages
Lack of Fit
If the patient has previously been appropriately instructed, they will hopefully realise themselves that their Hawley or vacuum-formed retainer (VFR) is not fitting properly. This can occur because, through wear and tear, the VFR plastic has ‘given’ a little or clasps have loosened up on a Hawley retainer (Figure 9.1). If this is the case, the patient will hopefully contact their orthodontist or dentist, i.e. whoever is responsible for monitoring and maintaining their retainer wear, so that adjustments or re-makes can be made as appropriate.
Figure 9.1 An Adams’ clasp that has become loose (a, arrowed) through regular wear of a modified Hawley retainer. The labial bow has been soldered to the bridges of the Adams’ clasps on this retainer. The clasp has been adjusted and tightened (b).
(Photographs courtesy of Simon Littlewood and Carol Bentley.)

Lack of Alignment
Of course, changes in alignment may occur through lack of fit, since a patient may fail to return in time for adjustments/re-makes. It is likely that any changes in alignment in these circumstances would have to be accepted unless an operator is either prepared to re-treat or there is scope to use a vacuum-formed active appliance (VFAA; see Chapter 11) to re-align very minor changes. However, the risk is ever present that changes in alignment can always re-appear in the future and it is simply not realistic for any patient to be on a potentially endless treadmill of re-treatment; nor would this be justifiable from the dental health perspective.
In contrast, minor changes in tooth position occurring over long periods of time may be less obvious to the patient as they see their teeth every day. It is not intended that patients wear their retainers full time forever. Therefore, nights-only or alternate-night wear can allow some tooth movement. Of course, patients may occasionally forget to wear their retainer too. These are the reasons why one cannot guarantee that there will never be any tooth movement – even when a patient is wearing a retainer (Figure 9.2) and regardless of whether a retainer is of the removable sort or bonded. The problems associated with bonded retainers are described below. Again, the main way of dealing with this problem is by explaining to the patient/parent/guardian at the initial consent stage what can (and cannot) be expected of treatment. Retainers may minimise tooth movement, but cannot be guaranteed to eliminate the possibility of all tooth movement.
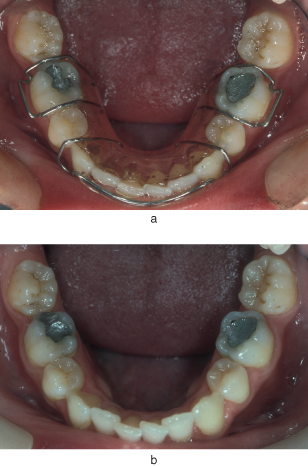
Figure 9.2 Example of minor tooth movement occuring despite reliable, alternate-night Hawley retainer wear. (a) With retainer; (b) without. These movements gradually became evident after about 2 years of regular retainer wear.
Discomfort
Removable retainers may rub the sulcus or gingivae, particularly following initial fitting. Most commonly for a lower Hawley this occurs in the lingual sulcus. Patients should be encouraged to continue wearing the retainer, but to return as soon as possible to have it eased. This provides the maximum chance of the operator being able to see the exact location of the problem, so trimming and easing can be carried out to greatest effect. Furthermore, continuing wear means that the risk of tooth movement is minimised.
For Hawley retainers, easing can easily be undertaken with a straight handpiece and an acrylic bur. For VFRs, rubbing or irritation is likely to occur against the gingivae. Easing of VFRs is described in Chapter 8.
Lack of Patient Motivation
If a patient fails to wear a retainer as instructed, there is probably little that can be done other than to warn them of the likely consequences of their actions, i.e. the teeth are likely to move out of position and this would have to be accepted.
Of course, lack of patient motivation may demonstrate itself in other forms, e.g. poor dental health maintenance or broken appliances. These problems will be dealt with elsewhere.
Breakages
If the patient notices any retainer breakage, then they should report back to their clinician as soon as possible for a repair or re-make as needed. Clearly, if an appliance is broken, it cannot maintain the alignment of the teeth appropriately (Figures 9.3 and 9.4).
Figure 9.3 A labial bow breakage. The labial bow has fractured at its solder joint to the bridge of an Adams’ clasp of a modified Hawley retainer. Clearly, alignment could be compromised until repair can be undertaken.
(Photograph courtesy of Simon Littlewood.)

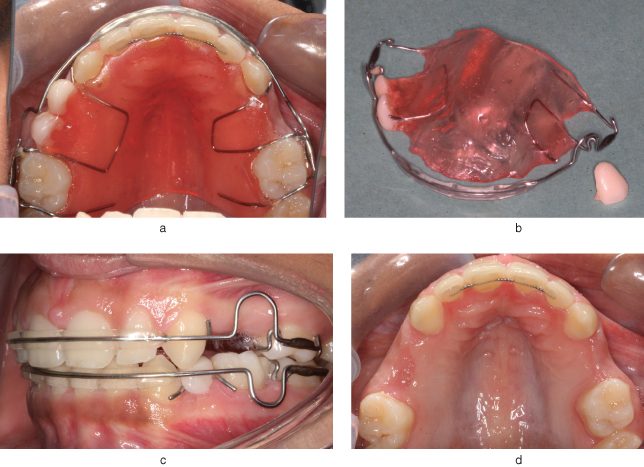
Figure 9.4 A Hawley retainer, modified with acrylic teeth, to maintain space and appearance until bridges or implants can be placed (a–d). In this case, a false tooth has fractured off the appliance (a–c). However, tooth movement into any spaces has been minimised, though not eliminated, due to use of a bonded retainer (d) and use of wire stops and clasp fly-overs (a–c).
(Photographs courtesy of Simon Littlewood.)
It is important that the clinician treating the patient establishes whether the breakage has occurred simply through wear and tear (e.g. one breakage occurs following a long period of good wear) or through carelessness or lack of motivation. If the latter, a discussion should take place with the patient/parent/guardian to ensure that they are fully aware of the repercussions of their actions and that further repairs/re-makes cannot be guaranteed regardless of any other factors. In rare cases it may be necessary to terminate treatment (see below for a discussion of managing retention/treatment termination).
Problems the Patient Is Unlikely to Be Aware Of
Dental Health: Caries and Periodontal Problems
Removable retainers, as with any appliance in the mouth such as a partial denture or bridge, will automatically increase the oral bacterial load and plaque retention factors. Therefore, caries and periodontal disease are a greater risk in patients with retainers. This is true regardless of the fact that the appliance can and must be removed to allow oral hygiene measures to take place. However, this does not mean the patient’s oral hygiene and care with diet (the latter from the caries point of view) will automatically be good.
Removable retainers, therefore, do have an advantage over fixed retainers in that they can be removed for cleaning. Despite this advantage however, it should not be assumed that dental health cannot be affected. Specifically, areas that can be especially affected are those that are hidden (or comparatively so) from the patient’s view, e.g. palatal surfaces, upper incisors, upper and lower gingival margins. Once gingival swelling occurs, it becomes more feasible for plaque to build up sub-gingivally. These issues explain why regular follow-up by the responsible clinician is essential for proper and thorough oral hygiene and dental health assessment and re-inforcement of need for good oral hygiene. Ultimately however, should oral health not improve, then consideration may need to be given to terminating retention (see below for a discussion of managing retention termination).
Problems with Bonded Retainers and Trouble-Shooting
As with removable retainers, the problems that can arise with bonded retainers can be grouped in a similarly convenient and clinically realistic way:
- Problems the patient is aware of
- Problems the patient is unlikely to be aware of.
All the problems that can arise, either directly or indirectly, ultimately affect whether or not alignment can be maintained and to what extent some level of misalignment has to be accepted. In the case of bonded retainers however, there is probably an increased risk that dental health could be compromised too.
Problems the Patient Is Aware Of
- Lack of alignment
- Discomfort
Lack of Alignment
Unfortunately, because the bonded retainer is always out of the patient’s direct view, the patient is unlikely to realise that there is a problem until they notice a tooth or teeth are no longer aligned.
This will usually be caused by one or more of the following breakages indirectly causing lack of alignment.
- A composite ‘blob’ debonds from the palatal or lingual surface of the tooth. This may affect one or more composite bonds and, therefore, several teeth may be free to move. In our experience, this is the most common cause of retainer breakage. See Figure 8.5 for an example.
Rarely, the patient may have heard a small ‘crack’ as the debond occurs or may detect a different ‘feel’ with their tongue. In these cases, the patient will hopefully return to have their bonded retainer checked and repaired as needed before any malalignment occurs. - Wire fracture. In our experience, this is not very common, but if it does occur one or more teeth are free to move (Figure 9.5). Once again, the patient may be aware of a change in the ‘feel’ of their retainer when they run their tongue over it, but commonly the patient will be oblivious of any problem until some tooth movement occurs. How­/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


