Chapter 9
Positive Pressure Irrigation
Cesar de Gregorio
Department of Endodontics, University of Washington, Seattle, WA, USA
Carlos Heilborn
Private Practice, Asunción, Paraguay
Nestor Cohenca
Department of Endodontics and Pediatric Dentistry, University of Washington, Seattle, WA, USA
Introduction
The foundation of endodontic therapy is the debridement and disinfection of the root canal system. These procedures would allow the clinician to achieve the ultimate endodontic goal: to preserve the health of apical tissues or to eliminate the apical inflammatory disease when it has already established as a consequence of bacterial colonization of the root canal system (1).
Our relentless pursuit to eliminate all irritants within a root canal system remains a committed objective. Unfortunately, our ultimate goal to completely disinfect every root canal system has not yet been practical. Predictable elimination of microorganisms remains our main challenge and has not changed significantly since 1965 (2). The terminology of disinfection as opposed to sterilization is appropriate as a result of the shortcoming in our objective. Although “cleaning and shaping” are done concurrently, disinfection actually begins after the desired shape has been accomplished (3). Traditional endodontic techniques are based on the theory that files shape and irrigants clean (4). Said differently, there is greater potential to completely disinfect the root canal system after it has been cleaned and shaped. This statement highlights the knowledge that there are uninstrumentable areas of pulpal anatomy. Studies confirm that better microbial removal and more effective irrigation occur when canals are instrumented to larger apical sizes (5–7). However, even after cleaning and shaping, microorganisms found in biofilm structures remain in the root canal system and dentinal tubules.
The efficacy of intracanal irrigation has been evaluated and reported extensively in the endodontic literature (8–13). Sodium hypochlorite (NaOCl) is considered to be the most effective irrigant solution because of its antimicrobial and tissue dissolution properties (10, 13–15). However, sodium hypochlorite must be in direct contact with the tissue to be disinfected in order to oxidize, hydrolyze, and to some extent osmotically draw fluids out of the tissues (16). This means enabling the sodium hypochlorite to contact the dentinal tubules throughout the complex root canal anatomy at working length (WL), as well as the anatomic variations like lateral canals and isthmuses (Figure 9.1).

Figure 9.1 Irrigation of a complex anatomy. Presence of an accessory canal in middle third. Irrigation was performed in a cleared tooth using apical negative pressure.
From the early days of endodontics, the objective of achieving an aseptic root canal was pursued using disinfectants applied to the coronal portion of the canals. However, the persistence of apical pathoses demonstrated that the entire length of the root canal system required exposure and contact with the chemical irrigant in order to provide for adequate disinfection. The first delivery system into the root canal was a needle connected to a syringe, currently termed positive pressure (PP) irrigation. The basic concept and clinical aim is to deliver the irrigant solution into the entire root canal, while generating a hydrodynamic flow to facilitate the removal of debris through the canal orifii. The latter is essentially aimed at avoiding accumulation and packing of debris produced during the instrumentation, particularly at the apical third, causing mechanical blockage and facilitating the growth of microorganisms and biofilm formation.
PP irrigation uses a syringe and a needle. The technique involves inserting the needle into the canal followed by the deposition of the irrigant solution. It is the most traditional technique and still considered the “gold standard” for endodontic irrigation (17–19), despite the questionable results reported in the current literature (15, 20–22).
Better understanding of fluid dynamics is required in order to understand the chemophysical properties directly correlated to the flow of irrigants in a closed-end canal system. By learning the physical limitations of fluid dynamics, we will realize that the delivery system is perhaps equal or even more important than the irrigant solution itself. This statement is supported by a number of in-vitro studies analyzing the efficacy of irrigants on dentin disks in which the solutions easily contacted the surface to be treated (23–25). Sodium hypochlorite has extraordinary qualities for disinfection and organic tissue dissolution. In combination with chelating substances such as ethylenediaminetetraacetic acid (EDTA), the disinfection should become more predictable, at least from a direct microbiological standpoint. Unfortunately, the clinical situation is very different and complex because of physical, chemical, and anatomical constraints. Therefore, it is unreasonable to extrapolate the results of in-vitro studies, when they do not replicate the clinical situation. Recently, the importance of using a closed-canal system was demonstrated by Parente et al. (26). We must realize and accept the fact that we are facing a challenging clinical situation ruled by physical principles. This challenge is further complicated by the chemical principles and limitations of irrigation solutions. The surface tension and viscosity of the irrigant produce a phenomenon known as dead zone or stagnation zone at the apical level in which the irrigant penetration is limited, making the renewal of the solutions virtually nonexistent.
The irrigant exchange achieved at the apical third when using PP irrigation is critical for the disinfection and removal of debris (11, 27, 28). Understanding fluid dynamics within a closed-canal system surrounded by apical tissues is extremely important when evaluating the goals of irrigation (Figure 9.2).

Figure 9.2 Penetration of sodium hypochlorite and a dye marker in a cleared tooth model where artificial lateral canals were created. Image (a) shows an open system with penetration into lateral canals and up to working length while image (b) shows a closed system with limited penetration at the tip of the needle.
Positive pressure: the technique
PP irrigation basically consists of syringes and needles inserted into the canal while pressure is applied to distribute the irrigant solution to the entire canal system. The only difference between this procedure and injection is that during root canal irrigation, the solution should enter and exit via the same orifii. This technique is quite a different clinical reality than inserting an injection where the objective is the insertion of liquid into the body with a syringe.
The syringe comprises a piston and a cylinder and is connected to a needle on one end using Luer lock connection that twists onto the needle hub for secure attachment and a leak-free connection. The alternative is to use a simple friction connection that may leak following elevated pressure generated by the piston, resulting in the leakage of the irrigants over the patient and operator.
Taking into consideration that the needle is the most influential component in this delivery system, few studies have analyzed the dimensions and correlation with ISO standards. Although instruments used in endodontics had been the subject of several studies for decades (18–20), this correlation was not analyzed until recently when Boutsioukis et al. (29) concluded that units of the widely used “gauge” system cannot be directly extrapolated to clinical practice. Thus, knowledge of the tip’s external diameter is crucial for the selection of the appropriate size irrigation probe during endodontic treatment.
The level of penetration of the needle is critical to the efficacy of PP irrigation. Wedging of the needle into the canal space should always be avoided in order to prevent accidental extrusion of the irrigants into the apical tissues (22, 23). A clinical dilemma is determining the apical preparation size required to match the needle’s gauge allowing deeper and safer penetration.
Stainless steel needles ranging from 21 to 30 G were analyzed and found in compliance with that of ISO 9626:1991 and 9626:1991/Amd 1:2001 specifications (29). However, the only NiTi needle analyzed, the Stropko Flexi-Tip (Vista Dental Products, Racine, WI, USA), exceeded the external diameter limits. The researchers observed deficiencies on the internal surface in all needles, regardless of the material or the manufacturer. This factor could directly affect the irrigant flow. The main concern raised by the study was the discrepancy between the needles’ gauge and the ISO standardized sizes in any specific point, probably because of the great variability of the particular designs. The variability identifies a lack of standardization in the manufacturing process. We must consider that the displayed gauge could be variable at different levels within the needle but not specifically in its most apical section.
Factors affecting efficacy of positive pressure irrigation
Closed systems: the physical challenge
In endodontics, a closed system means that the portal of exit of the root canal system, including lateral canals, apical foramen, and accessory foramina, is surrounded by vital apical tissues, creating a permeable but closed system. The clinical implication is that the irrigant solution must be delivered through the canal orifice, flow and exit back via the same orifice. The only way to overcome that “virtual barrier” would be to elevate the flux ratio and consequently the intracanal pressure (30). This will result in the extrusion of toxic irrigants to the apical tissues eliciting an inflammatory response with necrosis of the affected area and edema (31).
There are case reports in which the dissolution power of NaOCl produced severe effects on the medullar bone tissue (24), as well as permanent sequelae such as asymmetries and paresthesia (25). A recent publication (32) reports a clinical case in which a “sodium hypochlorite accident” was evaluated using 3D imaging (CBCT, cone beam computed tomography) to assess the degree of injury and possible anatomical reasons for the extrusion. This case illustrates once again that the risk of extrusion is real, even in cases in which low pressure is applied during PP irrigation. In this particular clinical case, the apex was fenestrated and not covered by buccal cortical bone. This anatomical variation demonstrates that the integrity of apical bone structures plays a decisive role on the containment of endodontic irrigants. Bone resorption is always expected, to a certain degree, in apical periodontitis and should be a concern for the clinician. This finding was highlighted by Salzgeber in 1977 (33), who demonstrated that the probability of irrigant extrusion was higher in cases with necrotic pulp and apical periodontitis. The loss of integrity of apical tissues and the fact that necrotic pulp tissue is less intact than a vital pulp, or even nonexistent in some cases, facilitates a free flow of irrigants to the apical end of the root canal. Recent studies by Vera et al. (34–36) using a similar methodology analyzed the dynamics of irrigants using the needle of smaller gauge. Their result concluded that irrigant penetration is very limited during root canal treatment and it is also conditioned by the formation of gas bubbles that get trapped at the apical or even middle third. This gas bubbles, produced primarily by ammonia and carbon dioxide liberation during pulp tissue dissolution, are termed vapor lock.
Patency
In a series of studies, Vera et al. (34–36) analyzed the effect of patency files on NaOCl penetration using a radiopaque contrast media. The studies concluded that maintaining apical patency did not have a significant effect on irrigant penetration at the apical third, even when canals were prepared to a size 30/09. Passive ultrasonic irrigation (PUI) had a positive result with more irrigant flow at the apical third. This data is in accordance with the results obtained with cleared teeth (37), where PUI demonstrated significant better results than PP on irrigant penetration to WL. Figure 9.3 shows penetration of NaOCl mixed with a dye marker using PP followed by activation with PUI in cleared teeth (Figure 9.3). Conversely, there are studies demonstrating satisfactory action in teeth with very similar preparations (12). This could be the result of different methodologies.
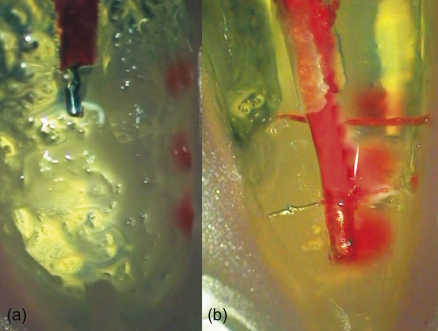
Figure 9.3 Penetration of sodium hypochlorite in cleared teeth: irrigant delivered using positive pressure (a) and activation of the solution with PUI (b).
The maintenance of patency in teeth with apical diameters greater than 30 was analyzed by Vera et al. (34), and the results demonstrated that patency maintenance with an #10 ISO file improved apical penetration of irrigants but only with great apical preparations. Thus, further apical enlargement could play an effective role in irrigant penetration, but this comes at the expense of apical transportation in 56% of the cases, according to the results of Goldberg et al. (38).
Apical diameter and taper of preparation
In a classic histological study, Senia (39) demonstrated the limited efficacy of sodium hypochlorite on the dissolution of organic matter at the apical third and isthmus areas of mandibular molars. This study confirmed that the size of apical preparation is determinant and directly related with irrigant penetration, getting more irrigant penetration in large apical preparations. The main strength of this study is that despite not being a current study, the author performed the investigation using a complete closed system design in an attempt to reproduce the flow dynamics of the clinical environment.
Vera et al. (34) observed that when apical preparation reached 40/06, the use of small diameter (#10 ISO) allowed for a significant improvement in irrigant penetration to WL. The #10 hand file did not show any effect in smaller apical diameters.
Increasing apical size allows better apical penetration of the irrigant and a greater renewal rate. Chow (11) described the difficulties for PP to exert a flushing action beyond the tip of the needle and the lack of action at the apical third. In this study, using glass tubes and a gel simulating pulpal and dentinal debris produced during canal preparation, a clear correlation was observed between the insertion depth of the needle and the flushing action of the irrigant.
Healing of apical lesions has also been demonstrated to be significantly better when apical preparation was enlarged to 3 ISO sizes over anatomical apical diameter, determined by the first file to bind at length (40). Although the research was not aimed at analyzing possible correlation between apical size, irrigation, and healing, we can assume that removing more contaminated dentin and allowing better apical irrigation contributed to the positive outcome.
Taper also plays an important role when irrigating with PP (41), but not for apical negative pressure (ANP) (discussed later in this chapter), which depends more on the ability to place the micro cannula at WL (42).
The influence of patency on gas and air bubbles is discussed in the following section.
“Vapor lock” phenomenon
The physical phenomenon of vapor lock is caused by gas entrapment, especially at the apical third of the root canal, impairing the access of irrigants to the whole extent of the root canal system. It is caused by one of the principal properties of sodium hypochlorite, the dissolution capacity of the organic component. This process leads to the formation of carbon dioxide and ammonia in the root canals, producing small bubbles that prevent the penetration and renewal of irrigants at the most apical levels.
Currently there are many studies analyzing this phenomenon. The first group to study this physic-chemical challenge was Tay et al. (43). Using a closed system, they analyzed the penetration of the irrigation solution (combined with cesium chloride (CsCl) as contrast) using scanning electron microscopy (SEM). The study highlighted the limitation of PP irrigation to remove debris from the apical third, even when the irrigant was delivered at 1 mm from WL. The only delivery system that was not affected by the vapor lock was ANP (Figure 9.4) (26). Figure 9.5 shows the vapor lock phenomenon (see arrow) affecting the PP irrigation (Figure 9.5).
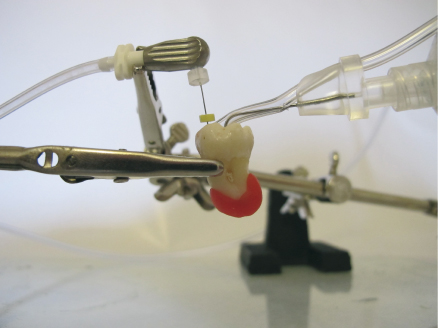
Figure 9.4 Apical negative pressure irrigation using microcannula of EndoVac at working length while the irrigant is delivered in the pulp chamber with the Master Delivery Tip.
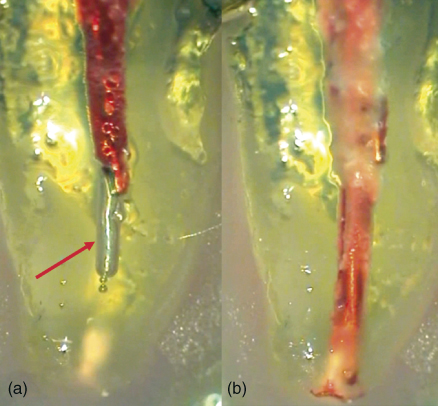
Figure 9.5 Vapor lock (white arrow) does not allow irrigant penetration up to working length when positive pressure is used (a) while apical negative pressure eliminates gas entrapment (b).
Recently, another study analyzed the presence of vapor lock in correlation with the apical diameter and needle design (44). The results were in agreement with other studies reporting the presence of apical gas entrapment in 48% of the cases while using PP irrigation. Increasing the apical size, using an open-ended needle, positioning the needle closer to WL, and delivering the irrigant at higher flow rate appeared to result in smaller vapor lock in-vitro. When this recommendation is extrapolated to the patients, increasing the flow rate at 1 mm from WL will elevate the apical pressure and expose the patients to irrigant extrusion, severe irritation of apical tissues, and consequently pain. Safety, efficiency, and predictability must be the main factors to consider when selecting PP or a different irrigant delivery/activation system.
The degree of root canal curvatures directly affects the penetration of the irrigation needle and consequently restricts the irrigant flow at the apical portion. The number of studies analyzing the efficacy of irrigation in curved canals is limited (45–47). The presence of slight curvatures, starting from 25°, represents a clinical challenge (48). Taking into consideration that the majority of clinical cases present with mild or greater curvatures, it is necessary to further study this major limitation and possible techniques to overcome.
In a microbiological study, the decreased effectiveness of PP in curved canals was demonstrated using bioluminescent bacteria (46). This study presented very relevant data concerning the physical limitations of the efficacy of needle irrigation. It was observed that in 24–28° curvatures, the differences obtained in the removal of the biological substrate were significant and correlated with the preparation size. Larger preparation sizes resulted in better apical irrigation.
When comparing PP with other activation systems or simultaneous combination of PP and activation, it was demonstrated that PP irrigation alone was not enough to obtain an adequate cleaning of the apical third (43). Conversely, when combined with activation systems like PUI, the results were significantly better, regardless of the curvature. A recent study confirmed that the action of PUI allows for irrigation at least 3 mm ahead of the ultrasonic file, even in curvatures greater than 50° and with 5 mm radius (49). Munoz and Camacho-Cuadra (50) evaluated irrigant penetration in-vivo, using a radiopaque contrast material. Mesial roots of mandibular molars were instrumented to 35/05 and a 27 G needle was positioned at 2 mm from WL. PP failed to irrigate at full WL while PUI and ANP obtained significantly better results.
Despite the available evidence regarding the advantage of using hybrid techniques for root canal irrigation (i.e., combining PP with PUI or sonic activation), Dutner et al. (51) reported that almost half of the clinicians do not use any coadjutant system while irrigating with PP.
Methods used in the analysis of irrigant penetration
Different methods have been employed for fluid dynamics and apical irrigation research, including the thermal image analysis proposed by Hsieh et al. (41), which employs a technology never used before in endodontics. This method consists of a temperature distribution analysis among oral tissues and is commonly employed in oral pathology research (52). The energy emitted by an irrigant solution heated to 50 °C and placed into root canals of teeth previously cooled up to 10 °C was analyzed. With this method, the level of the solution extension is known with relative accuracy. It was observed that a minimum apical preparation to ISO size #30, along with the placement of a 27 G needle up to 3 mm from WL, was needed to detect temperature changes in the last millimeter of the samples. Contrary to what we might deduce for larger diameter preparations (over ISO #80), equivalent to teeth with immature apices, the efficacy of irrigation does not increase, but decreases because of the turbulence generated in the root canal during irrigation, which prevents the solution to reach the complete preparation length.
Between 2009 and 2011, various papers have been published (37, 53, 54) that reported analyses in an in-vitro model to evaluate irrigant penetration in real time with different devices, including PP. This model used cleared teeth with the external surface sealed with wax, creating closed systems in which contrast colored sodium hypochlorite was visualized. This model allowed visualization of the entire canal length and for standardization of noninstrumented, artificially created lateral canals of 60 µm in diameter.
The main conclusion from these studies is that PP, compared with different delivery and activation systems, does not accomplish the objective of delivery of the irrigant to WL and to difficult access areas as lateral canals. In the three papers published with this methodology, PP was not able to reach the results obtained with ANP (EndoVac®) for WL penetration, and the results obtained with PUI for noninstrumented areas.
Computed fluid dynamics (CFD)
In 2009, a new method for irrigation analysis was introduced. The computed fluid dynamics (CFD) has been used in engineering for many years, and more recently in medicine, to analyze blood flow patterns in circulatory pathologies (55) or breathing flow conditions (56). This technology overcomes limitations of previous methods used in the study of fluid dynamics (57–60), which provided only macroscopic assessment and very general information.
CFD allows one to obtain data about fluid speed, something inconceivable in an experimental model. Information about fluid speed, intracanal pressures, and stress over canal walls can be easily gathered with this technique. The first CFD analysis focused on the effect of irrigant fluid speed during final irrigation using a 30 G side-vented needle on the flow pattern produced in a root canal instrumented to 45/06.
In this computational analysis, the irrigation needles were measured to determine the internal and external diameter and the incidence and degree of deviation from ISO 9626:1991 and ISO 9626:1991/Amd 1:2001 specifications (29). Root canals were standardized to 19 mm length with continuous 6% taper and apical diameter ISO #45 (0.45 mm), based on the results of a final 45/06 K3 file (Sybron Endo). At the apical level, an apical constriction was tridimensional constructed as an inverted cone, to better simulate the clinical situation of a natural root canal. This anatomy design was based on a previous study by Ponce and Vilar Fernandez (61) that described a maxillary central incisor.
For the irrigation process, the irrigation needle was placed 3 mm from WL and centered in the root canal. For fluid speeds, data from the 2007 study were used (29). For the design of irrigant fluid, density, viscosity, and specific gravity of 1% NaOCl were applied, and the root canal was considered impermeable, closed at the apical end and full of fluid.
Fluid movements on delivery by the needle depended on the speed applied and marked a 30° angle trajectory from the side port exit surrounding the needle tip and forming a vortex into the apical zone. The current flowed laterally through the side port at the maximum speed producing reduced irrigant replacement at the apical zone of the root canal. Even when greater flow speeds were applied, the irrigant could not advance more than 1 mm ahead from the needle tip. Only with very intense flow speed rarely used in clinical procedures because of extrusion risk it was possible to achieve 1.5 mm ahead from the needle tip. Besides the intracanal irrigant speed data, relevant information was obtained relative to the mechanical efficacy of close-ended and side-vented needles, particularly related to the irrigant stress produced over the dentinal wall at the exit site level. The term stress is directly related to the “flushing” phenomenon, responsible for the debris removal effect. From this study, it was concluded that the removal of debris attached to the canal wall would be more efficient in the areas near the side port.
There are currently some disadvantages in this method of studying irrigation using computational models, for example, the absence of dentinal chips, pulp tissue. The friction between the fluid and dentinal walls is also absent. The simulated root canal is completely closed apically, without extrusion risk. From this first study by Boutsioukis et al. fluid dynamics acquires an important role in the field of irrigation. For this reason, six more studies were later published with similar methodology. We discuss two of these for methodology validation.
In a study by Gao et al. (62), the aim was to identify the turbulence mode that best reproduces the clinical situation, comparing the results obtained by CFD with the observation of in-vitro simulation. Instrumentation of a methacrylate resin block was used to simulate a prepared root canal in-vitro (Endo Training Block; Dentsply Maillefer, Ballaigues, Switzerland). The blocks were instrumented to an apical size of 30/09, corresponding to a ProTaper F3 file, and the foramen was sealed with modeling wax in order to create a closed system. The prepared root canal was reconstructed by computer to perform the CFD analysis using a micro-CT scanner in order to obtain an exact reproduction. Comparing this model with the one used by Boutsioukis et al., we find that the main difference (besides root canal preparation) is the presence of curvature. The needle used by Gao et al. is also different, as the 28 G side-vented Max-I-Probe had a wider caliber.
The identification of the efficacy of this model was one of the objectives; considering that the flux of distillated water used as irrigant is considered laminar, it changes to turbulence following the lateral exit and collision with the canal wall. The second was to analyze if the model was able to correctly identify the “dead water” or “stagnation zone” area. After comparing CFD results with those recorded by a macro mode video camera during irrigation with water stained with a dye, they concluded that from the different turbulence models applied, only one, SST k-u, corresponded with the in-vitro
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


