8
The aetiology of malocclusion:
(i) skeletal and soft tissue factors
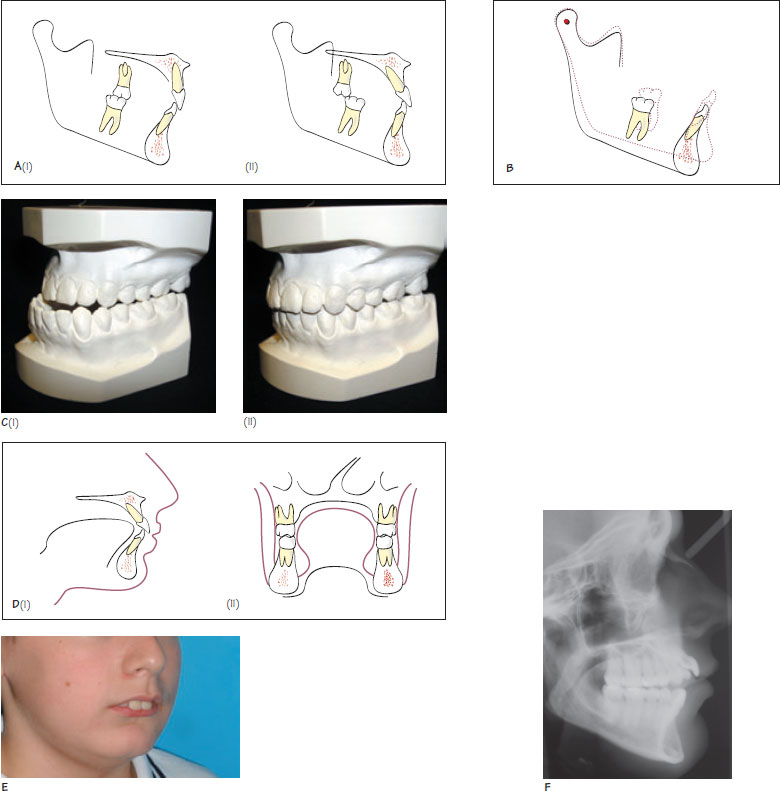
Figure 8.1 (A) Dento-alveolar compensation. Under the influence of favourable soft tissues, in Class II malocclusions (i) the lower incisors may be proclined and the uppers retroclined, and in Class III malocclusions (ii) the upper incisors may be proclined and the lowers retroclined to compensate for the sagittal skeletal discrepancy. (B) Interaction between the anteroposterior and vertical dimensions. Downwards and backwards rotation of the mandible results in a reduction of chin prominence. (C) The interaction between the anteroposterior and transverse dimension. Before treatment (i) there is a bilateral buccal crossbite. Treatment involving maxillary advancement (ii) has resulted in spontaneous correction of the crossbite as a wider part of the maxilla has been moved forwards relative to the mandible. This is an example of a relative transverse maxillary discrepancy. (D) Light, prolonged, resting forces placed by the lips, cheeks and tongue determine the position of the dental crowns above their apical base (equilibrium theory). (E) An example of a lower lip trap where the lower lip is trapped behind the upper incisors at rest. This can result in upper incisor proclination and retroclination of the lower incisors. (F) Anterior tongue posture. The tongue is clearly seen protruding between the insisors and making contact with the lips at rest. This may have contributed to the development of the increased curve of Spee in the upper arch and the anterior open bite.
An understanding of the aetiology of malocclusion is important in the prevention and stable correction of occlusal discrepancies. Malocclusion is due to a combination of genetic, or inherited, and environmental factors. The relative importance of each of these depends on the trait under examination. From a clinical perspective, it is useful to classify the aetiology of malocclusion under the following headings: skeletal factors; soft tissue factors; dento-alveolar or local factors; and habits.
Some of these factors are inter-related, for example the skeletal pattern can influence lip position. Commonly the aetiology of malocclusion is multifactorial.
Skeletal factors
Skeletal factors should be considered in three planes.
Anteroposterior
The anteroposterior (AP) relationship of the maxilla and mandible can have a large influence on the sagittal occlusal relationship. If the soft tissues are favourable, the incisors may compensate, by proclination or retroclination, for a given skeletal discrepancy. This is termed dentoalveolar compensation (Figure 8.1). In such cases, the occlusal discrepancy will appear less severe than the underlying skeletal defect. If the soft tissues are unfavourable, the malocclusion may appear worse than the underlying skeletal discr/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


