37
Anchorage management
Table 37.1 The magnitude and duration of headgear forces required for anchorage reinforcement, distalieation of maxillary molars and maxillary restraint.
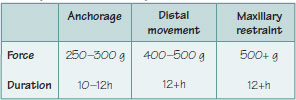
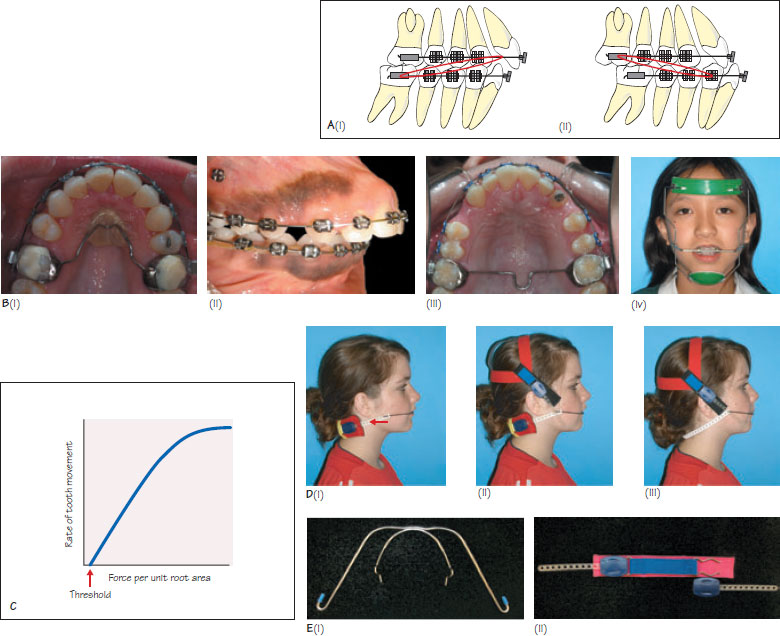
Figure 57.1 (A) Intermaxillary traction. (Í) Class II elastics run from the lower molars to the upper incisors. They aid upper incisor retraction and mesial lower molar movement whilst maintaining the upper molar and lower incisor position. There is also an extrusive force placed onto the lower molars and upper incisors, (ii) Class III elastics run from the upper molars to the lower incisors and encourage lower incisor retraction and mesial movement of the upper molars whilst maintaining the position of the upper incisors and lower molars. (B) Anchorage appliances. Clinical examples (i) Nance palatal arch, (ii) mini-screw implants (iii) transpalatal arch and (iv) protraction headgear. (C) The relationship between the force per unit area of root surface and the rate of orthodontic tooth movement (differential force theory). A threshold force exists below which no tooth movement occurs. (D) Examples of headgear (i) low (cervical) pull with a neck strap, (ii) straight pull using a head and neck strap and (iii) high pull using a head strap. The red arrow shows the Masel safety strap. (E) Components of headgear: (i) the Kloehn bow, (ii) snap-away elastic modules. The neck strap, head strap and Masel safety strap (arrow) are shown in Figure (Di).
Anchorage maybe defined as resistance to the unwanted three dimensional forces generated in reaction to the active components of an appliance. The reactive forces are equal and opposite to the active forces according to Newton’s third law of motion (every action produces an equal and opposite reaction). Poor anchorage management can result in a non-ideal occlusion, over-retraction or under-retraction of the incisors, and poor facial aesthetics.
Anchorage requirements should be assessed by space analysis during treatment planning (Chapter 18). If 75–100% of extraction space is required for the correction of malocclusion, anchorage requirements can be considered to be high.
Classification of anchorage devices
Anchorage devices can be classified according to the tissue(s) providing resistance to unwanted tooth movement.
Intra-orally the teeth, skeletal structures and soft tissues can provide anchorage. When the teeth are used, the anchor unit should incorporate as many teeth as possible, so that the force threshold needed to initiate tooth movement is not exceeded. Teeth from the opposing dental arch can also be used to provide inter-arch anchorage with Class II or III intermaxillary elastics (Figure 37.1A). The bone covering the palate can be a useful source of anchorage because of its large surface area. Removable appliances and the Nance palatal arch (Figure 37.1Bi) commonly use the palate as a source of anchorage. More recently, skeletal anchorage has become increasingly popular with the introduction of implants and mini-screws (Figure 37.1Bii). These devices provide maximum anchorage, unlike previously mentioned methods, which means that space loss is />
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


