23
Class II division 2 malocclusion
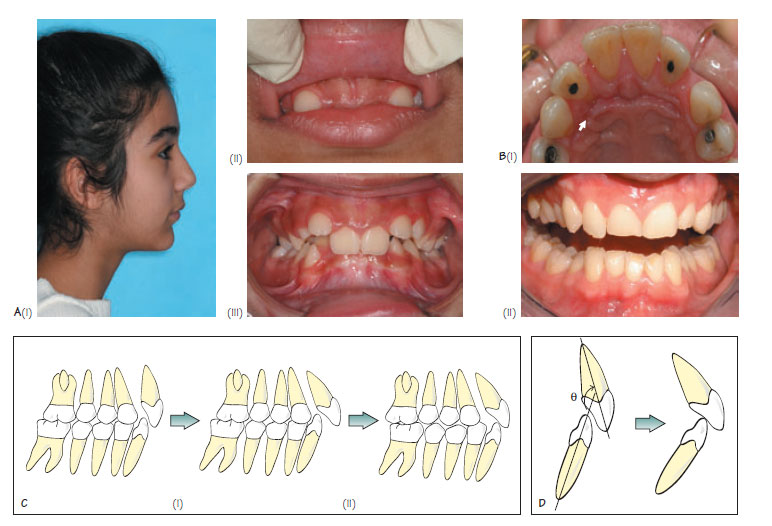
Figure 23.1 (A) Some features of Class II, division 2 malocclusion: (i) mild mandibular retrognathia, with a pronounced chin point and reduced lower anterior face height, (ii) high lower lip line, and (iii) retroclined maxillary central incisors and deep overbite. (B) Traumatic overbite leading to (i) periodontal damage on the palatal aspect of the upper right lateral incisor and (ii) severe attrition. (C) The management of Class II, division 2 malocclusion with functional appliances involves (i) proclining the maxillary incisors into a Class II, division 1 relationship, which allows forward posturing of the mandible, and (ii) correction of the overjet. (D) Reduction of an increased interincisal angle is important for stable overbite correction.
Class II division 2 is the term used to describe a malocclusion where the lower incisal edges occlude posterior to the cingulum plateau of the upper incisors and the upper central incisors are retroclined (British Standards Institute classification). The overbite (OB) is characteristically deep, the overjet maybe normal or increased, and the molar relationship is Class II. There is an association between this malocclusion and impacted maxillary canines. The prevalence of Class II division 2 is estimated to be approximately 10% among Caucasians. This malocclusion has a strong genetic association.
Aetiology of Class II division 2 malocclusion
Skeletal factors
Class II division 2 is commonly associated with a mild skeletal II pattern due to mandibular retrognathia. The chin point may be well positioned in a number of cases with retrusion more evident at the dento-alveolar region (Figure 23.1Ai). A moderate/severe skeletal II pattern may be present, however, is more likely to be associated with a Class II division 1 incisor relationship as the lips are more likely to be incompetent. Class II division 2 may rarely be associated with a skeletal I or III relationship if the soft tissue pattern is unfavourable.
Vertically, the lower anterior face height (LAFH) and Frankfort-Mandibular planes angle is often reduced (Figure 23.1Ai). This maybe associated with an anticlockwise (forward) mandibular growth rotation (see Chapter 5). A reduction in the LAFH predisposes to a high lower lip line, deep OB and a pronounced labiomental fold.
In the transverse dimension, there may be a scissor bite in the premolar region which is a result of narrowing of the lower arch and because a wider part of the maxilla opposes a narrower part of the mandible (relative transverse discrepancy, Chapter 8).
Soft tissue factors
As a result of the reduced LAFH, the lower lip usually rests high on the crowns of the maxillary central incisors (Figure 23.1Aii). A high lower lip line results in retroclination of the maxillary central incisors, an increase in interincisal angle and deepening of the OB (Figure 23.1Aiii).
A deep labiomental fold
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


