8
Prosthodontics
Urgent care in prosthodontics is a frequently neglected subject in dental school curricula, textbooks, or field publications. Yet, inevitably the clinician is faced with a patient whose prosthesis has failed and is in need of urgent treatment. Often the dental laboratory is relied upon to help solve the problem; however, this requires removal of the restoration and several working days—a consequence ill-tolerated by many patients. Fortunately, this situation can frequently be avoided, at least temporarily.
This chapter outlines both definitive and temporary solutions for some of the more common urgent problems associated with complete dentures, removable partial dentures, and implants. The repair procedures that follow can be accomplished in the dental office with a minimum of equipment and supplies. Some of the procedures are considered to be temporary, but will allow the patient functional ability until more definitive treatment can be accomplished.
Fractured Artificial Teeth
Tooth and Segments Present
Fracture and separation of anterior artificial teeth is probably the most common complete denture emergency, but it is also one of the most easily remedied. Repair is easiest if the residual artificial tooth (or teeth) can be recovered. Since the base-tooth interface is the weakest point of the restoration, the tooth breaks cleanly from the base and can be precisely repositioned (Fig 8-1). Even when the fracture involves the body of the tooth, if it can be repositioned precisely it can be repaired so as to be virtually undetectable.
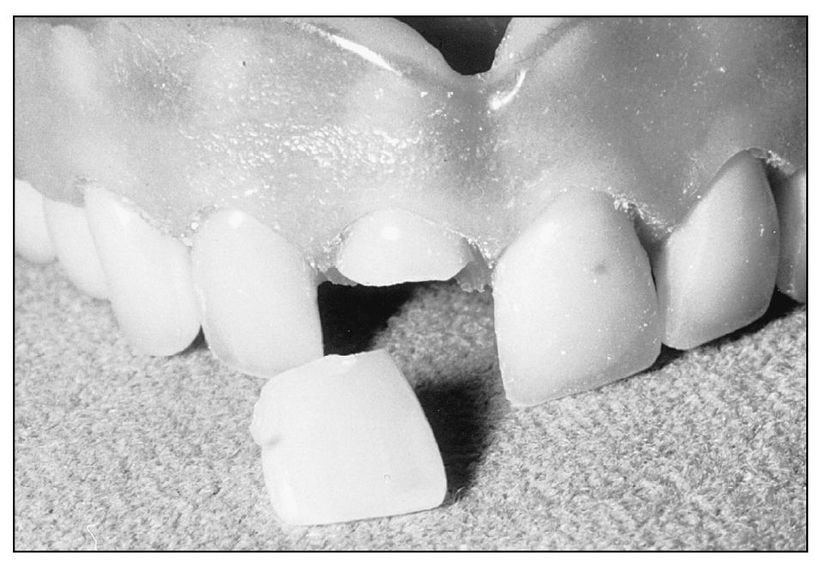
Fig 8-1 Typical clean fracture through the body of an artificial tooth.
| Step 1 | Clean the fractured segments of debris and interfering fragments . Often the segments will precisely relate. Reposition the smaller segment and temporarily fasten using sticky wax, tracing compound (Fig 8-2), or cyanoacrylic cements (eg, Superglue). |
| Step 2 | Apply a layer of quick-setting plaster to the facial surface of the denture to create a removable matrix. |
| Step 3 | Separate the tooth/segment to be repaired from the base and reposition precisely with the matrix (Fig 8-3). (Free positioning the segments invites errors and increases rather than decreases the total time.) |
| Step 4 | Slightly roughen the acrylic resin surface with a bur to promote chemical bonding of the repair resin. Remove a generous amount of base material to easily introduce the repair acrylic resin. If possible, try not to remove resin from the facial aspect of the fracture site to prevent fluid resin from running onto the esthetic aspect of the denture. |
| Step 5 | Treat the matrix with a separating agent (liquid detergent in water works well) and reposition the tooth/segment and fasten (with sticky wax) to the denture. |
| Step 6 | The repair autopolymerizing acrylic resin is then applied by wet ting the prepared surfaces with monomer and polymer in a “salt and pepper” fashion, and allowed to cure. Density and speed of curing can be maximized by the use of a pressure pot and hot water, although this apparatus is not essential. |
| Step 7 | Verify the occlusion and polish the repaired prosthesis. Inform the patient that the repair acrylic resin will change color with time. |
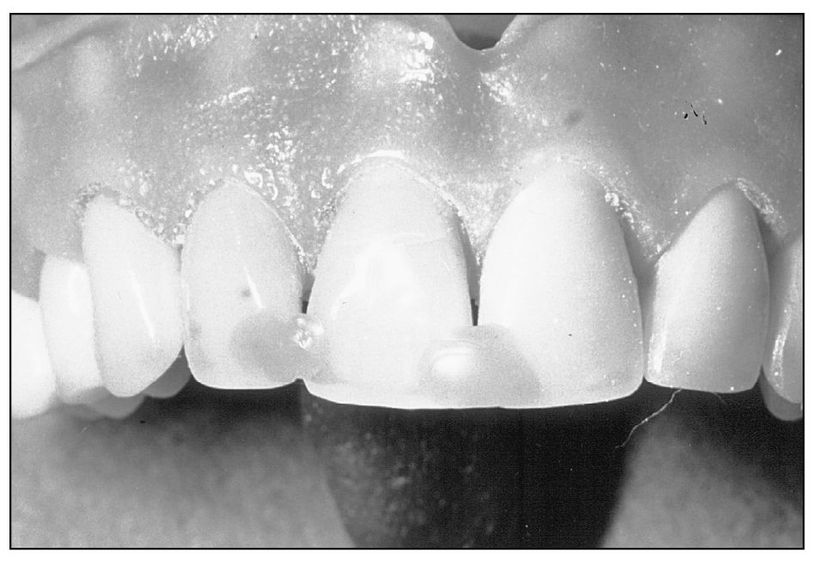
Fig 8-2 Fractured segment is repositioned using sticky wax.
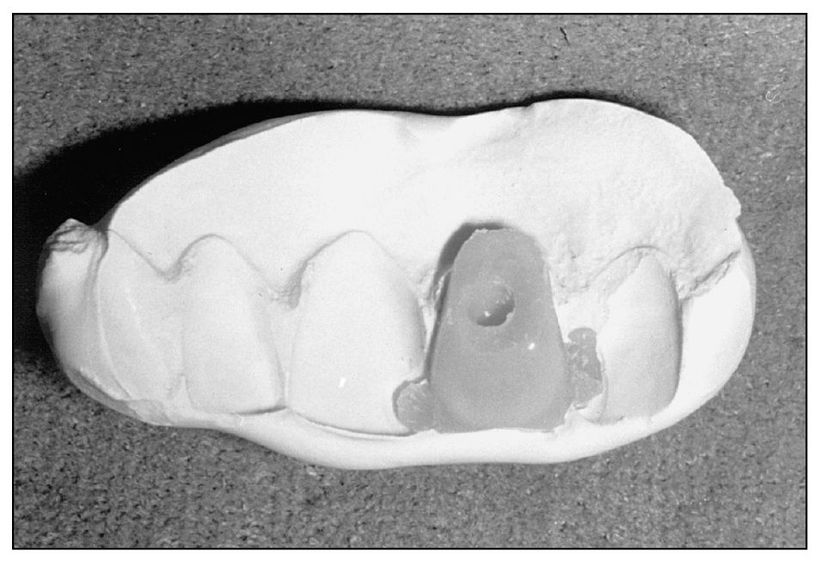
Fig 8-3 Lingual view of positioning matrix of quick-set plaster.
Fractured Denture Base
Denture base fractures vary from simple chips or cracks in flanges to multiple through-and-through fractures of the entire base. Most common is the single through-and-through anteroposterior fracture of the base. In restorations with acrylic resin teeth, the fracture may split or otherwise damage a tooth. Usually, such fractures result from dropping or stepping on the denture; however, fatigue fracture is frequently associated with a denture opposing a full compliment of natural teeth.
Simple Fracture
| Step 1 | When the base or flange has fractured cleanly into two pieces (Fig 8-4), repair is often quick and simple, without the need for laboratory procedures; however, the denture is retained for several hours. The fracture allows for complete and precise apposition of the segments, which are temporarily affixed with sticky wax, tracing compound, or cyanoacrylic cement (eg, Superglue). Be sure the segments fit precisely together. |
| Step 2 | Apply a matrix of quick-set plaster (or half quick and half regular to slow setting time) to the tissue surface of the reassembled base. Block out severe undercuts in the denture base with wet pumice, soft wax, or wet tissue paper. Allow the matrix to set for several minutes to gain strength. Quick set plaster will be sufficiently strong in 10 minutes. |
| Step 3 | Using appropriate burs, widen the fracture, creating a trough for application of the repair autopolymerizing acrylic resin. This trough must be narrowed at the interproximal area of the dental and facial component of the restoration to minimize esthetic detractions. (If an artificial tooth must be replaced at the same time, make the base repair first, and then position the artificial tooth as noted earlier in this chapter.) |
| Step 4 | If the fracture involves the facial surface of the base, the use of slightly different color than the repair material can be esthetically displeasing if the repair trough is too wide. Therefore, it may be necessary to repair this region in from the tissue surface in a second stage, after the majority of the fracture has been repaired. The partially repaired denture is removed from the plaster matrix and the facial fracture trough is carefully widened from the tissue surface, leaving the facial segments virtually untouched and minimizing the exposed repair resin. |
| Step 5 | The repair autopolymerizing acrylic resin is “salt and peppered” into the prepared fracture site and allowed to cure. |
| Step 6 | The repaired restoration is then tried-in, and the fit of the base is confirmed to be pressure free with the use of a pressure-indicating substance. Additionally, since subtle alterations in base segment position can dramatically affect the occlusion, a careful evaluation of the base segment position must be done before dismissing the patient. |
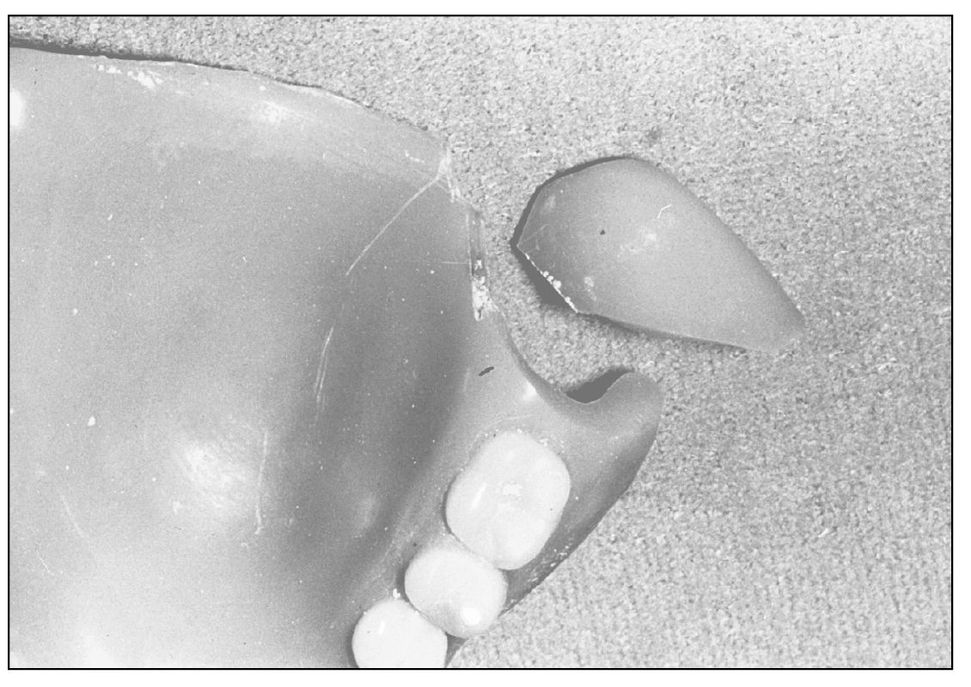
Fig 8-4 Simple denture base fracture. The segments can be repositioned precisely for quick repair.
Complex Fracture
If the majority of the base and flange can be repositioned intraorally, then often repair can be made, despite sizable missing pieces (Fig 8-5).
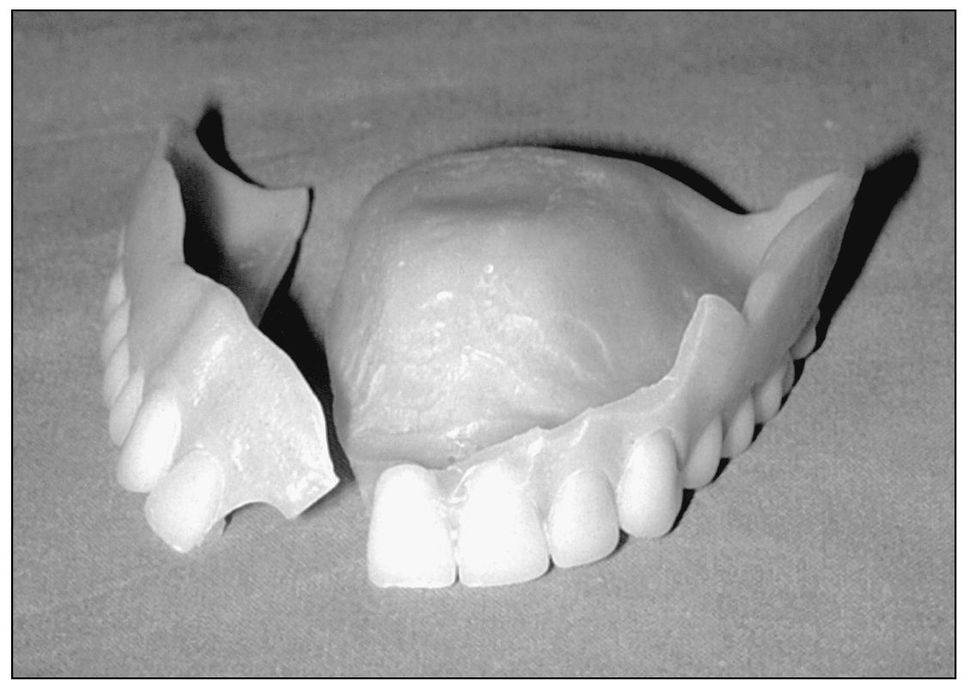
Fig 8-5 A more complex fracture of the denture base and labial flange, but one that can still be repaired in the office.
| Step 1 | Assemble the major fractured base segments so that they can be consistently positioned intraorally—both from a tissue and an occlusal perspective. Missing portions—such as flanges or other segments—can be created intraorally with the use of various border molding materials and/or waxes. The material Tak (Tak Systems) readily adheres to the segments and has a relatively prolonged fusing time thus permitting intraoral repositioning of the segments. |
| Step 2 | Transfer the assembled segments to the patient. The opposing occlusion is used to guide the segments into proper position, and after the tracing compound has become rigid, the assembled restoration is then taken to the laboratory. |
| Step 3 | A plaster matrix is used to maintain the temporarily affixed segments of the prosthesis. The matrix maintains the fractured segments and creates the tissue surface of the lost flange. Quick -setting plaster works well and minimizes the waiting time to less than 15 minutes. |
| Step 4 | Widen all fracture lines with an appropriate bur and remove irregular edges. Remove all tracing compound or other residue from the fracture areas and widen them sufficiently to allow the repair material to flow onto the fracture sites. |
| Step 5 | Paint the plaster matrix with a separating agent and correctly reposition the segments. Autopolymerizing acrylic resin is then “salt and peppered” into the defects. Where a large volume of resin may be needed, using the pour technique to apply the acrylic resin may be quicker (Table 8-1). Place the prosthesis in the pressure pot and allow the acrylic resin to cure. The usual trimming and polishing can then be performed. |
| Step 6 | The completed repaired prosthesis is now returned to the patient and the usual verification of tissue surface and occlusion can be performed. |
Table 8-1 The Pour Technique
| The Pour Technique is used when large additions of acrylic resin are needed, such as the addition of a flange to an existing prosthesis. This technique works best on broad flat expanses. | |
| Step 1 | Depending on the extent of the area to be repaired, place approximately 5 to 10 mL of repair monomer liquid in a 30 mL plastic medicine dispensing cup. |
| Step 2 | Squeeze enough repair resin into the monomer liquid to produce a mixture with the consistency of cream (ie, dispense about twice as much powder as liquid). |
| Step 3 | Pour the liquid mixture into the prepared site. With practice, it is possible to control the distribution of the mixture. |
| Step 4 | Using a gloved finger dipped in monomer liquid for lubrication, smooth and contour the area. |
| Step 5 | Correct areas of deficiency with subsequent mixes of acrylic resin or by using the “salt and pepper” technique. |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


