9
Orofacial Lesions
Pain in the oral cavity is not an unusual complaint of dental patients, and most of the time, that pain can be attributed to obvious disease processes that directly affect the dentition (eg, caries, pulpal pathosis) and/or the periodontium. However, the pain may not always be associated with the teeth or the periodontium but may be due to oral lesions that are affecting other oral tissues. Sometimes these orofacial lesions can cause severe pain and compromise the patient’s ability to masticate, swallow, and even sleep; in other instances, these lesions may be a source of great concern, especially for the cancerphobic individual. Therefore, the dentist must make every effort to accurately diagnose the patient’s problem and either provide a cure or symptomatic relief.
Squamous Cell Carcinoma
Squamous cell carcinoma (SCC) of the oral cavity is an invasive malignant neoplasm of the epithelium of the mouth and oropharynx. It is predominantly found in males aged 50 to 70 and females aged 60 to 80 years, with a very strong relationship to alcohol and tobacco use/abuse. The incidence of SCC is twice as high for males as females. Ninety-seven percent of all intraoral SCCs are found in three high risk areas of the oral cavity: floor of the mouth (50%; Fig 9-1), soft palate complex (32%), and ventrolateral surface of the tongue (18%). On the floor of the mouth, over 70% of the lesions found there are located in the anterior portion.
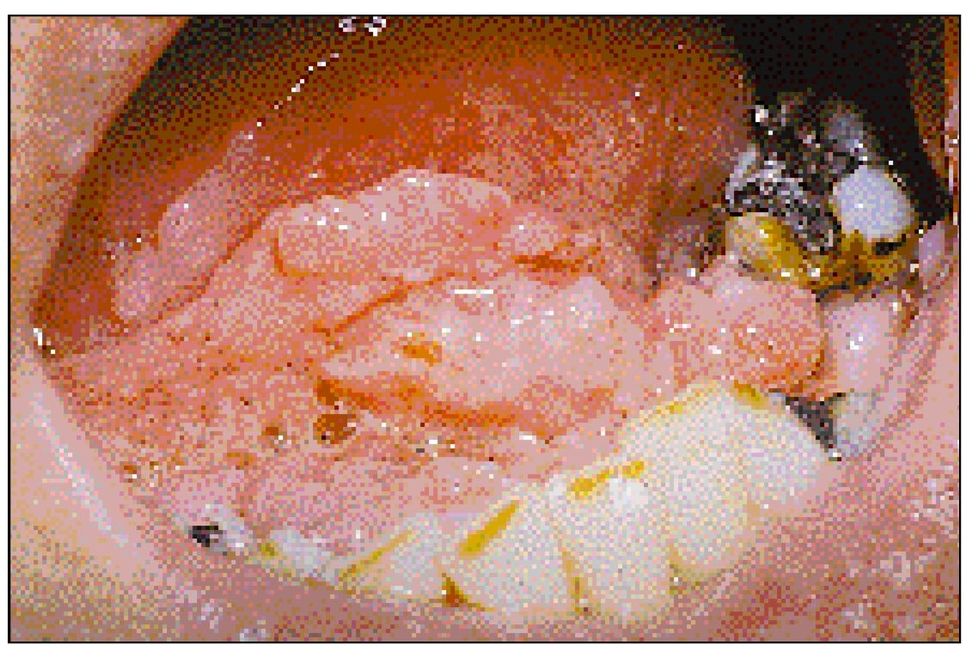
Fig 9-1 Stage III squamous cell carcinoma on the anterior floor of the mouth in a 48-year-old male with a history of tobacco and alcohol abuse.
Signs and Symptoms
Early SCC, leukoplakia, and/or erythroplasia is usually asymptomatic (Fig 9-2). If the carcinoma does cause signs and symptoms, the patient will complain of pain, bleeding, ulceration, a mass, or difficulty in swallowing. Unfortunately, the lesion at this point is at least a stage II disease, often with associated lymph node involvement.
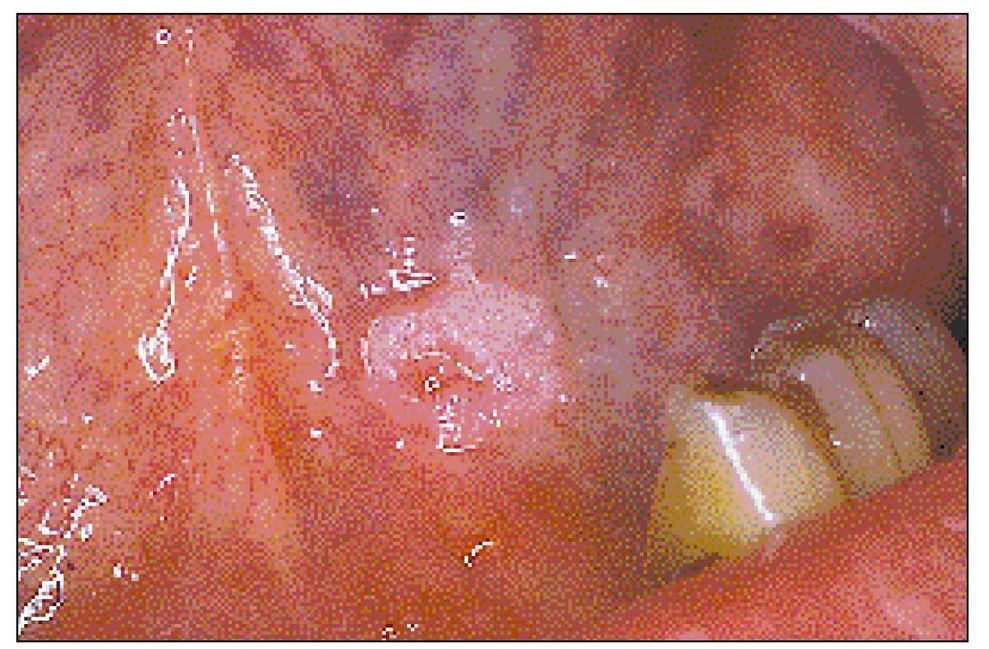
Fig 9-2 Stage I squamous cell carcinoma on the anterior floor of the mouth in a 51-year-old male with a history of alcohol abuse.
Traumatic Ulcers
The traumatic ulcer is an oral ulcer that is the direct result of an injurious event. Some common sources of trauma are sharp restorations, fractured teeth, orthodontic wires, ill-fitting dentures, thermal injury (hot or cold), chemical injury, and factitious injury (self-inflicted).
Signs and Symptoms
The border of the ulcer is irregular with an erythematous halo of variable width surrounding a gray-yellow crater (Fig 9-3). The ulcer can occur on any mucosal tissue, but is more commonly found on the buccal mucosa, tongue, floor of the mouth, and palate. The ulcer may or may not be painful or may only be painful while eating. The ulcer will heal in 7 to 14 days without scarring.

Fig 9-3 Traumatic ulcer. Lesion of unknown traumatic origin located on the left floor of the mouth adjacent to the mandibular left premolars. Note the irregular margin and the narrow, distinct erythematous halo.
Recurrent Aphthous Stomatitis (Oral Ulcers)
Recurrent aphthous stomatitis (RAS) is the most common ulcerative disease of the oral mucosa. The etiology is unknown; however, suspected predisposing factors include (1) local trauma, (2) microbial infections (eg, streptococci, varicella, and cytomegalovirus), (3) systemic conditions (eg, nutritional deficiencies and/or malabsorption syndrome resulting in decreased serum levels of folic acid, iron, and B-complex vitamins), systemic illnesses resulting in decreased immune status (HIV), (4) genetic factors (RAS may occur along family lines), and (5) immunologic factors (increased serum immunoglobulins; possible cell-mediated immune response).
Signs and Symptoms
Minor aphthae are usually less than 5 mm in diameter and are located on the labial and buccal mucosa, soft palate, and tongue and heal without scarring (Fig 9-4). Major aphthae are greater than 5 mm in diameter, are present for up to 6 weeks, and often heal with scarring. The lesions most often occur on the lips, soft palate, and tonsillar fauces resulting in severe difficulty in chewing and swallowing. Herpetiform ulcers usually begin in the third decade of life and are characterized by multiple ulcers (2 x 3 mm in diameter) that can occur anywhere in the oral cavity. These ulcers may coalesce to produce larger ulcers with irregular borders.

Fig 9-4 Recurrent aphthous ulcer. A classic representation of the minor aphthous variant, this lesion is located on nonkeratized alveolar mucosa and has a regular margin with a diffuse erythematous halo.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


