7
Relationship between Abutment Geometry and Peri-implant Tissue in Esthetic Zone Cases
Department of Oral Health and Rehabilitation, School of Dentistry, University of Louisville, Louisville, KY
Introduction
Dental implants have proven to be predictable long-term treatment options for optimizing the support, stability, and retention of dental prostheses. This has resulted in a greater acceptance of dental implants as important components of care by both patients and clinicians. There has been a concurrent rise in the expectations of optimal outcomes, both functional and esthetic.
In order to increase the predictability of a satisfactory treatment outcome, particularly from the esthetic perspective, provisional and definitive implant-based restorations must achieve several goals:
- They must harmonize with the patient’s overall appearance and face.
- They must encourage a healthy intraoral environment.
- They must imitate the natural appearance of the adjacent dentition by reproducing the form, size, texture, and optical properties of the teeth being replaced (Buser et al. 2004).
Successful contemporary dental implant treatment is therefore not only defined by the survival of implants or the absence of biologic and prosthetic complications, but also, and importantly, by an optimal esthetic outcome. The esthetic result must satisfy even the most demanding clinical circumstances and patient. Optimal three-dimensional positioning of the dental implants is determined by rigorous pretreatment diagnosis and planning. Restoration-driven treatment has, for the most part, been embraced to effectively reduce the risk of a negative esthetic or functional treatment outcome (Martin et al. 2007).
Factors contributing to the overall esthetic result may include the anatomy of the implant sites (gingival biotype, shape of adjacent teeth, bone level at adjacent teeth), placement of the implants (oral–facial position, mesial–distal position, coronal–apical position, distance between tooth–implant or implant–implant), the hard/soft tissue management procedures during the implant treatments, and the design or prosthetic management of provisional/definitive restorations. This chapter will focus on the prosthetic management of tissues adjacent to the dental implant via provisional restorations, customized impression techniques, and definitive abutments and final restorations.
Provisional Restorations Prior to Implant Loading
General Considerations
Provisional restorations associated with implant therapy fall into two broad categories. First, there are those provisional restorations utilized between tooth extraction and implant placement/loading. Second, provisional restorations need to be supported by the implants subsequent to placement. Each form of provisional restoration plays a specific role in the achievement of satisfactory treatment results (Higginbottom et al. 2004).
The provisional restoration serves many purposes and provides several advantages when incorporated into dental implant-based treatments. Provisional restorations positioned subsequent to extraction and prior to implant placement provide patients with economic, esthetic, and functional replacements that are satisfactory in the short term. Provisional restorations used in this treatment phase should be durable and readily maintained. Further, they should lend themselves to simple removal and replacement, modification, and adjustment throughout the treatment process.
The clinician may also gather information relevant to the definitive treatment during the provisional restorative phase. This information may include tooth shade, restorative contours, and peri-implant soft tissue profile. Each of these parameters may also be used as a tool for communication between treatment team members, and between the treatment team and the patient. The ability of the patient to visualize and evaluate the proposed restorative outcome may be of great significance.
Soft and/or hard tissue augmentation is often an important aspect of the esthetics of implant-based treatment. Augmentation procedures may be undertaken to increase tissue volume, facilitating the placement of an implant and improving the likelihood of a stable long-term result. Augmentation procedures may be used to enhance esthetic conditions in areas where adequate volume for implant placement is present, but where the residual ridge contour is less than ideal from the esthetic perspective. Appropriately designed provisional restorations can enhance patient comfort and satisfaction during the lengthy healing periods associated with augmentation procedures. Further, duplicates of provisional restorations can allow the surgeon to visualize tissue deficits and the planned restorations.
Contouring of the proposed implant site can commence immediately following tooth extraction. The provisional restoration can be ovate in form to initiate the shaping of the future peri-implant soft tissue. This can be accomplished with removable or fixed provisional restorations, although removable provisional restorations should be used with caution, particularly in the presence of grafts.
Fixed provisional restorations offer several advantages in treatment based on dental implants. Fixed prostheses eliminate vertical pressure on the tissue, which is critical in protecting outcomes associated with augmentation procedures. Fixed provisional restorations are also associated with improved patient comfort and assessment of esthetic potential. Further, they may increase patient acceptance of implant treatment because of the satisfaction of psychologic demand. However, fixed provisional restorations often require longer chair time and higher degrees of clinical skill and experience, in addition to considerably higher laboratory costs.
In general, removable provisional restorations may be more straightforward to fabricate, often at a lower laboratory cost. For clinicians, removable restorations may also be easier to deliver and adjust. Removable prostheses can be borne by the tooth and/or soft tissue. Tissue-borne removable prostheses will likely be associated with increased and intermittent loading or pressure on the grafted or implant sites during the healing process. This may jeopardize the optimal result of augmentation or implant procedures. Further, poorly designed prostheses may have a negative impact on the final soft tissue result. Careful attention is therefore required with regard to fit and adaptation of removable prostheses.
Fixed Provisional Options
Phase I provisional restorations, utilized between tooth extraction and implant placement, are an important treatment step (Chee 2001; Priest 2006; Santosa 2007). They are used primarily to satisfy the patient’s masticatory and esthetic requirements. In addition, they maintain stability both within the dental arch, and with the opposing teeth. Provisional restorations used at this stage can, however, also be utilized to contour soft tissue and direct healing so as to improve the site for implant placement, and increase the likelihood of an optimal outcome.
The options for phase I provisional restorations include a cast metal or fiber-reinforced resin-bonded fixed prosthesis (RBFP) or a partial fixed prothesis.
Cast Metal or Fiber-Reinforced Resin-Bonded Fixed Prostheses
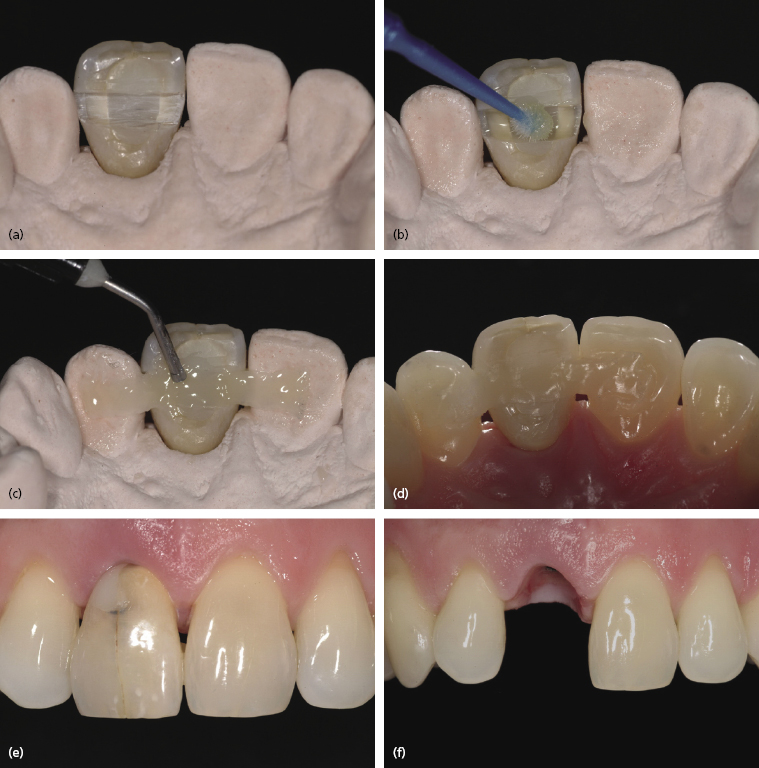
A RBFP with or without an ovate pontic may be used as a provisional or interim restoration if sufficient interocclusal space is available. Such space is needed both for occlusion and to contour the soft tissue prior to implant placement and/or loading. A RBFP offers the advantages of a fixed prosthesis – including superior patient comfort and control of pressure to adjacent tissues with minimal interference at the implant or graft site. Resin-bonded interim prostheses should only be in contact with small areas of etched enamel for retention on adjacent teeth. Pontic options include acrylic or composite resin denture teeth, metal-ceramic pontics (with cast metal frameworks), ceramic denture teeth or extracted crowns, and extracted natural teeth (Figure 7.1).
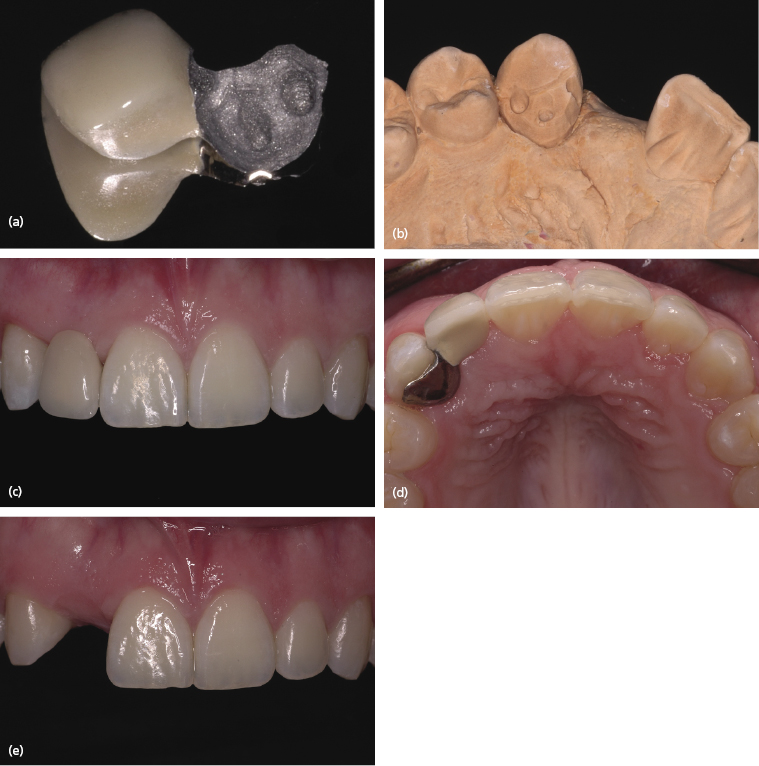
Each of these options can be modified to incorporate a cast metal or polyethylene ribbon designed as both reinforcement and as the prosthesis retainer. The laboratory costs may be substantial, most notably for a metal-ceramic RBFP (Figure 7.2).
The cost of a fiber-reinforced RBFP is relatively low. The procedure is also less complicated for both the technician and clinician.
Resin-bonded fixed provisional restorations are not recommended when multiple surgical procedures (extraction, ridge augmentation, implant placement, second stage surgery) are anticipated. Constant removal and repositioning may be detrimental to both the adjacent teeth and the provisional restoration. Fiber-reinforced options are, for the most part, not reusable subsequent to removal.
Partial Fixed Prostheses
In situations where full coverage restorations are planned for teeth adjacent to the implant site, these teeth can be used to retain and support provisional fixed restorations (Figure 7.3).

This option can provide a convenient and predictable provisional solution. The provisional restorations can be fabricated chairside or in a dental laboratory, and may be contoured to encourage tissue shape and healing. Although most prostheses of this type are fabricated using auto-polymerizing acrylic resin or composite, the dental laboratory may also process a more durable prosthesis with customized texture and shade using a heat-polymerizing material. This may provide a superior esthetic and functional outcome, although at a higher cost.
Provisional fixed prostheses can be fabricated prior to extraction and/or implant placement via the indirect method, so they are ready in time for the surgical procedure. This can make the treatment phase easier for the patient to tolerate. Pontic modification can also be done throughout the healing and tissue maturation period by adding or subtracting resin material from the tissue contact areas. As with alternative fixed provisional options, controlled pressure can be applied on the implant site to achieve optimal tissue contours.
Removable Provisional Options
Vacuum-Formed Removable Retainer Supporting an Ovate Pontic
A vacuum-formed removable retainer supporting an ovate pontic (Essix retainer) can be an effective and satisfying provisional restoration. Interocclusal space is often restricted and difficult to achieve before soft or hard tissue augmentation procedures. Provisional options other than the Essix retainer can be challenging to use. An Essix retainer is usually easy to fabricate, is relatively inexpensive, and can be a convenient option prior to making a longer lasting provisional prosthesis. A denture tooth, or extracted tooth, can be modified to fit the pontic site and to esthetically match the adjacent dentition. The tissue contact areas at the pontic site can be adjusted to an ovate shape in order to achieve optimal soft tissue contours. It can also be modified to be completely free of tissue contact.
A vacuum-formed appliance is tooth retained and supported, however it is still considered to be a removable prosthesis. Although it may provide the advantage of applying controlled pressure at the implant site, there are the usual disadvantages of a removable prosthesis. Patient compliance in wearing the prosthesis in order to continually contour the soft tissue at the implant site is important. Removable provisional options may be occlusally uncomfortable. They are, however, resistant to catastrophic fracture and are often readily accepted.
Interim Removable Partial Dental Prosthesis
Interim removable prostheses are commonly used as they are relatively inexpensive and easy to fabricate (
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


