46 Endodontics in the Mixed Dentition
Endodontic treatment in the mixed dentition involves the treatment of permanent teeth with incomplete root formation, a clinical situation that one often encounters in patients between 5 and 13 years of age. Following eruption of a tooth, it is another few years before root formation is complete and the apex is definitively developed. These teeth have a very high regenerative potential; however they can show an extreme reaction when exposed to infection.
The necessity for endodontic treatment in the anterior segment is usually associated with a complex posttraumatic situation. In the posterior segments it is usually the first molars that become problematic because of the effects of early caries or rapid posteruptive tooth substance loss due to disturbances of enamel formation (e.g., molar–incisor hypomineralization [MIH]).
Endodontic treatment is rendered more difficult by the usually irregular canal lumen and the lack of the apical barrier. Especially in younger children, limited cooperation must also be taken into consideration. If molars are affected, an orthodontist should be consulted before initiating endodontic treatment in order to clarify any possible space problems and the necessity for orthodontic extractions. In these cases, preferably deeply carious first molars should be extracted rather than sound premolars.
46.1 Anterior teeth
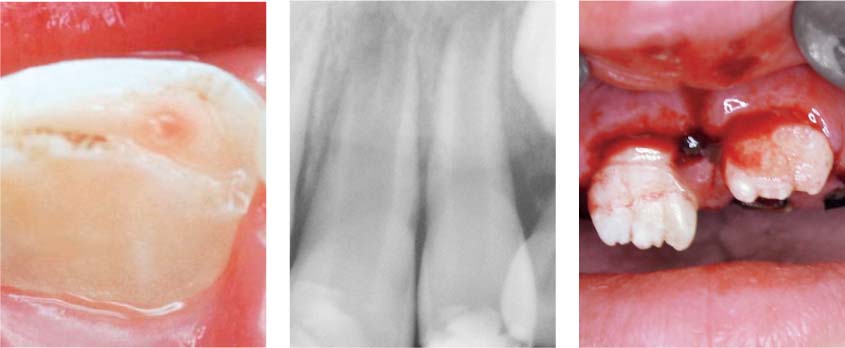
Left: Pinpoint pulpal exposure. The size and duration of pulpal exposure are decisive factors for further treatment.
Middle: Apical radiolucencies can be transient following trauma, and are referred to as “transient apical breakdown.” They must be differentiated radiographically from inflammatory induced alterations.
Right: Percussion or sensibility tests are not reliable indicators immediately following trauma, but should be regularly done during the course of treatment.
46.2 Molars
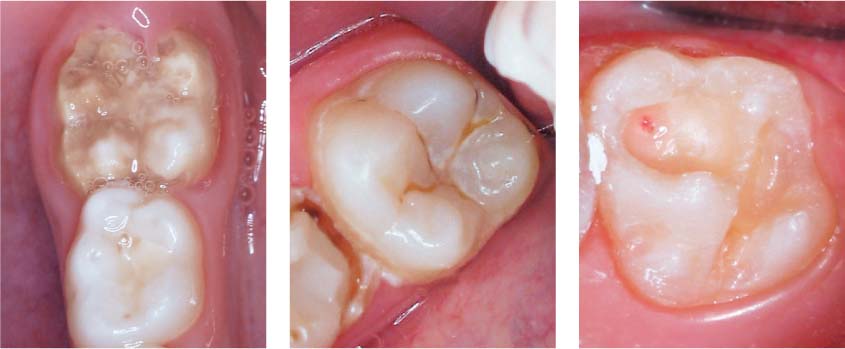
Left: Enamel malformations such as MIH can lead to early pulp exposure and the necessity for endodontic therapy.
Middle: A special problem is that of so-called “hidden caries”: intact enamel masks an extensive area of dentinal caries.
Right: During caries excavation, the pulp was exposed at the base of the cavity. The type of treatment for such an exposure depends on its size.
46.3 Caries diagnosis
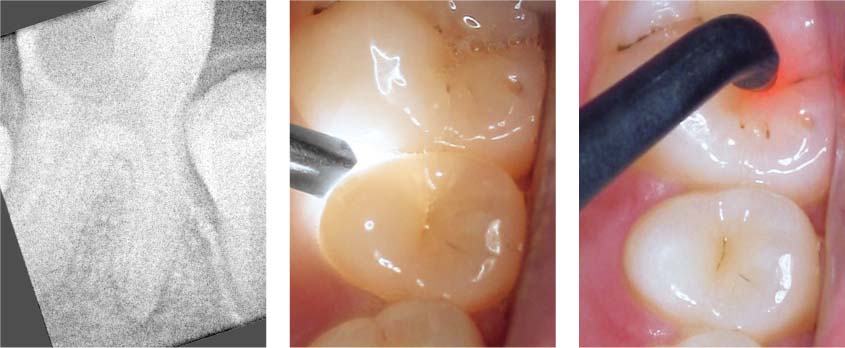
Left: Advanced caries. Radiographically it is often difficult to differentiate between periapical radiolucency and incomplete root development.
Middle and right: Early diagnosis is of special importance. Alternative methods include transillumination (middle) or laser-based caries detection (right).
Methods for Maintaining Tooth Vitality
The regenerative potential of the young pulp is extremely high, so that following indirect or direct pulp capping with calcium hydroxide, there is a good chance of subsequent hard-tissue deposition and therewith maintenance of pulp vitality. A more extensive pulp exposure can be treated by means of pulpotomy (similar to deciduous teeth).
Retention of the radicular pulp will ensure completion of the root development. In order to protect the pulp from contamination, an absolutely dry working field is critical. If the pulpotomy is successful, conventional root canal treatment will not be necessary later on.
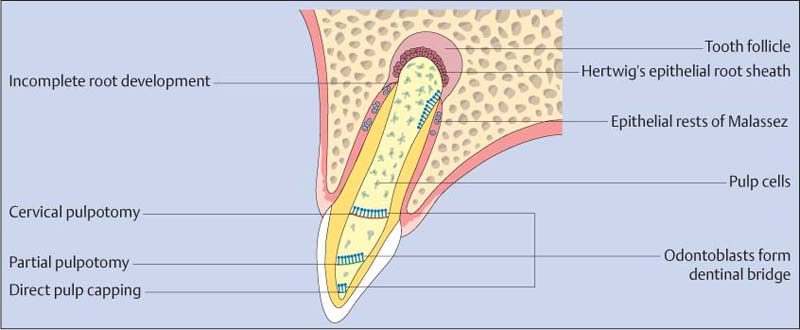
46.4 Histologic structures in teeth exhibiting incomplete root development
Direct pulp capping is only indicated in teeth with small (pinpoint) pulp exposures and a healthy pulp. If carious but hard dentin i/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


