Chapter 4
Surgery
Aim
The aim of this chapter is to discuss the basic planning and procedures for implant therapy.
Outcome
After reading this chapter the reader should be familiar with the precautions and procedures necessary to complete implant surgery to the required precision.
Introduction
To carry out precise and successful implant surgery, a thorough knowledge of surgical anatomy and a clear view of the planned prosthetic outcome is required. The surgical techniques described must be as atraumatic as possible to both hard and soft tissues.
Mandible
The main anatomical considerations when placing implants in the mandible include the:
-
inferior dental canal
-
mental foramina
-
submandibular fossae.
Inferior Dental Canal
The position of the inferior dental canal can be a major limiting factor when placing implants in the posterior mandible, as it may restrict the length of implant used. It is therefore essential to locate the canal accurately to allow optimal length of implant to be placed. To achieve this, high-quality radiographs are a necessary part of the preoperative assessment, and supplementary views may be required during the surgical procedure. Surgical exposure and identification of the mental foramen may be helpful in confirming the position of the canal (Fig 4-1).
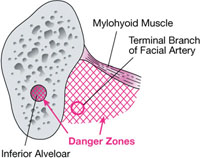
Fig 4-1 Cross-section view of posterior mandible showing where considerable care needs to be taken during surgery for implant placement.
Mental Foramina
The mental foramen defines the site where the inferior dental canal leaves the mandible. Anterior to the mental foramina, it is usually possible to place longer implants, given the amount of bone present. If, however, implants are to be placed close to the foramina, care must be taken that the inferior dental canal has not looped back on itself, leaving a section of the inferior dental nerve anterior to the foramen.
The incisive branch of the inferior dental nerve, which runs anterior to the mental foramen, may be damaged by implants being placed in the anterior mandible. Patients may occasionally comment on some altered sensation in the area. This is usually transient.
Submandibular Fossa
The submandibular fossa is lingually positioned to the body of the mandible below the mylohyoid line. The fossa may limit the placement of implants, especially in the posterior section of the mandible. The anatomical shape of the mandible in the region of the fossa varies considerably and in the posterior region may take the form of a thin lingual shelf through which the unwary may accidentally penetrate. The position of the mylohyoid line can usually be palpated with ease, although it is sometimes necessary to obtain a 3D scan of the area to define the exact shape of the mandible in the region.
The facial artery loops over the submandibular gland in the region of the first permanent molar and gives off a substantial terminal branch in the form of the submental artery. This is at risk of damage in the anterior aspect of the-fossa, possibly as far forward as the canine position.
Maxilla
The main anatomical structures to be alert to when placing implants in the maxilla are the maxillary antrum (Fig 4-2) and the incisive canal.
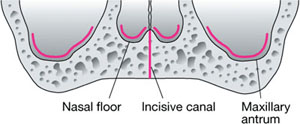
Fig 4-2 Surgical anatomy of maxilla showing sites where implant placement may be restricted.
Maxillary Antrum
The maxillary antrum is often a major limiting factor for the use of implants in the posterior maxilla, frequently making implant placement impossible without resorting to bone augmentation procedures. It is worth noting that, if planning to extract maxillary premolar and molar teeth before implant placement, the removal of the teeth may initiate “pneumatisation” of the antrum into the alveolar process. This results in a reduction in the bone available for implant placement.
Incisive Canal
The neurovascular bundle contained within the incisive canal is positioned in the midline, palatal to the central incisor teeth. If implants encroach on this canal, soft-tissue rather than hard-tissue union can be expected in this area. Depending on the extent to which an implant encroaches on the incisive canal, involvement of this anatomical structure may adversely influence the success of the implant placement.
Bone Quality
Bone quality is important in implant success. Typically, the ideal bone is of good vascularity with an adequate cortex and medullary bone of a reasonable density. The anterior mandible is generally considered to be a good site, although penetrating the dense cortex requires a very careful technique to avoid overheating of the bone. The posterior maxilla, which may have eggshell-thin cortex and a sparse medullary space, is generally considered to be the least favourable site for implant placement.
Surgical Technique
The procedure is carried out after careful planning and involves precise soft-tissue handling and bone preparation. The treatment is carried out under sterile conditions. It is essential that bone preparation is made as atraumatic as possible, with heat generation being minimised. Adverse cellular changes can occur within the bone with temperature increases of as little as 4°C. The technique therefore requires intermittent action, controlled operating pressures and copious amounts of saline coolant.
Implant Positioning
The position of implants is dictated by the intended position of the final restoration, n/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


