CHAPTER 4
Anterior Torque Control
“Success is the natural consequence of consistently applying the basic fundamentals.”
—Jim Rohn
Incisor Mandibular Plane Angle Position
In the 1950s, Charles Tweed revolutionized orthodontic diagnosis with the Tweed Triangle. The hallmark of this triangle was the position of the mandibular incisor in relation to the mandibular plane, or the incisor mandibular plane angle (IMPA).
Always aware of the IMPA in my early cases, I soon realized that Tweed’s 90-degree angulation could not be accurate in all patients. I began to question the position of the IMPA while in graduate school, especially after I traced my own IMPA position and found that it was 100 degrees. Surely Dr Tweed would not have extracted on my straight profile to achieve an IMPA of 90 to 95 degrees. Unfortunately, several years ago I heard an orthodontist justify his patient’s final concave profile by saying that he satisfied the Tweed Triangle. But which is more important in the end: the triangle or the face? Therefore, I eventually adjusted my thinking from the 90-degree concept to a more realistic goal for the IMPA.
My goal for IMPA today is called the 3-degree rule. It makes sense that the most stable position for IMPA in every patient is the position in which the patient presents. And experience has taught us that we can upright the incisors considerably and retain stability. So the major problem for posttreatment stability of mandibular incisors becomes their excessive advancement. When analyzing several long-term studies, I concluded that, in most cases, we should limit mandibular incisor tipping to 3 degrees.
Evidence
Several studies have used records from our practice to analyze the position of the IMPA. Glenn used a nonextraction approach to procline the mandibular incisors,1 moving them forward 1.4 mm; Elms successfully used nonextraction to tip the IMPA 2 degrees in crowded arches2; Alexander used extraction to measure the difference in mandibular incisor movement between stable and unstable groups,3 the former moving only 2.8 mm while the latter moved 4.7 mm; Nevant studied the effectiveness of a lip bumper in tipping the incisors,4 citing a movement of 1.4 mm per year, or 2.9 degrees; and Papandreas reported an 8-degree annual uprighting of the mandibular incisors in extraction cases.5 In another study, Hansen measured the effects of the Herbst appliance on the mandibular incisors, reporting that the appliance’s anteriorly directed forces on the mandibular premolars causes the mandibular dentoalveolar segment to move forward, thereby resulting in proclination of the mandibular incisors.6
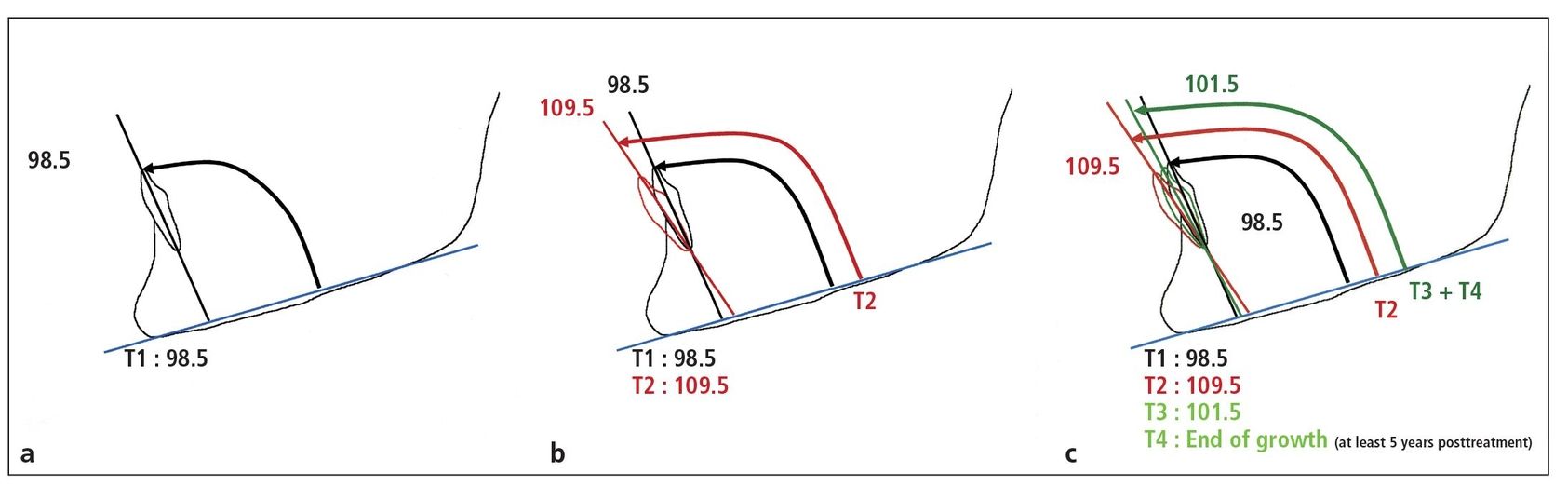
Fig 4-1 (a) Pretreatment IMPA position. (b) Final IMPA position. (c) IMPA position 5 years posttreatment.
The difference in mandibular incisor proclination between skeletal Class II correction with a cervical facebow and functional appliances such as the Herbst stems from Newton’s third law of relativity: For every action, there is an equal and opposite reaction. With a facebow, the opposite reaction occurs at the back of the neck whereas the opposite force for any intraoral appliance affects the entire mandibular dentoalveolar segment. Although these appliances effectively address skeletal Class II problems, they are deficient in controlling IMPA.
In the Hansen study, IMPA shifted from 98.5 degrees to 109.5 degrees, meaning the mandibular incisors flared 11 degrees. Yet when the patient stopped retention 5 years after treatment, the incisors were uprighted to 101.5 degrees, a permanent proclination of 3 degrees from the original position (Fig 4-1).
Mechanics
To control IMPA, attack the problem with exact bracket and archwire specifications:
- 0.018 slot
- –5-degree torque mandibular incisor brackets
- –6-degree tip on mandibular first molars
- Initial flexible rectangular archwire to give torque control
- And if needed:
- –Interproximal enamel reduction (slenderizing) to gain space
- –Early Class III elastics to upright molars
If crowding is so severe that a rectangular archwire cannot be engaged or if the treatment plan suggests that the incisors can be advanced, then a 0.016 nitinol (NiTi) mandibular archwire can be used.
A common mistake made by orthodontists is the use of open-coil springs between incisors to gain space, which causes flaring of the incisors. To reduce flaring, in addition to interproximal enamel reduction, Class III elastics (¼-inch 3-oz) can be worn for the first 3 days (72 hours) of treatment. This distalizing force can upright the mandibular first molars (which have a–6-degree angulation on the bracket) to gain space. Wearing the Class III elastics over a longer period can cause unwanted extrusion of the mandibular incisors, which is not advisable. At the next appointment, additional slenderizing will obtain better archwire engagement, and the patient can once more wear Class III elastics for 72 hours. This procedure can be used for up to 3 months.
As soon as the rotations have been reduced to the point where a 16 × 22 or 17 × 25 multistranded archwire can be engaged, the Class III elastics can be stopped. The torque of the mandibular anterior teeth is now controlled by the rectangular archwire and torque (–5 degrees) in the incisal brackets.
The trademark of the Alexander Discipline is the prescription of–5 degrees of torque in the mandibular central incisors. The torque values in the 0.018-inch slot brackets are designed to compensate for the 5 degrees of archwire freedom when a 17 × 25 stainless steel (SS) archwire is used. The resultant force is 0 degrees of torque expressed on these teeth. The–5 degrees of lingual crown–labial root torque compensates for the 0.001 inch of tolerance between the 17 × 25 archwire and the 0.018-inch bracket slot.
Fig 4-2 Patient with deep bite. (a) Pretreatment cephalometric tracing. (b) Posttreatment cephalometric tracing. Notice the change in IMPA.
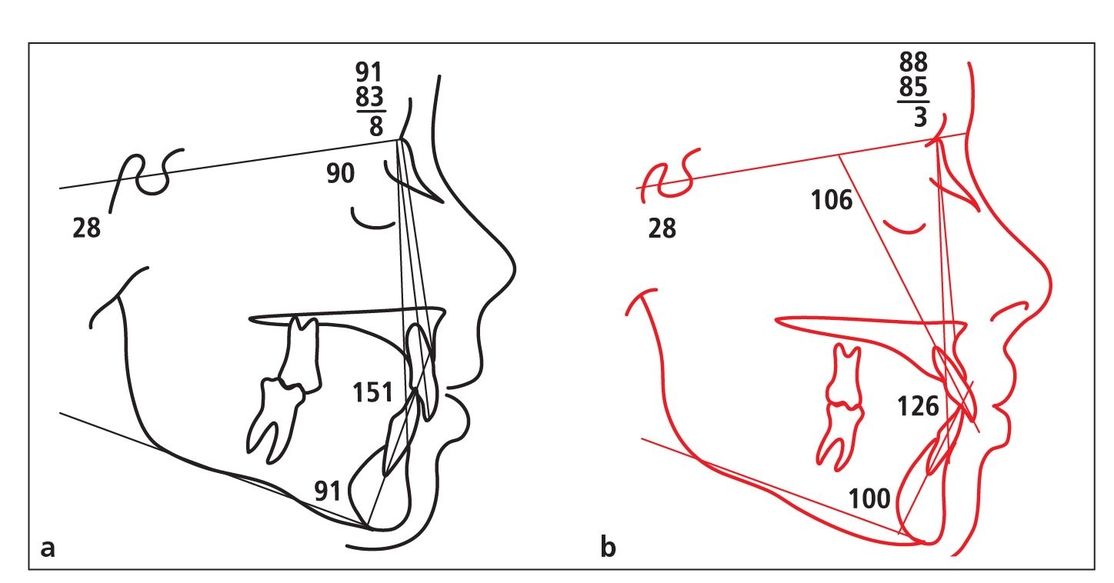
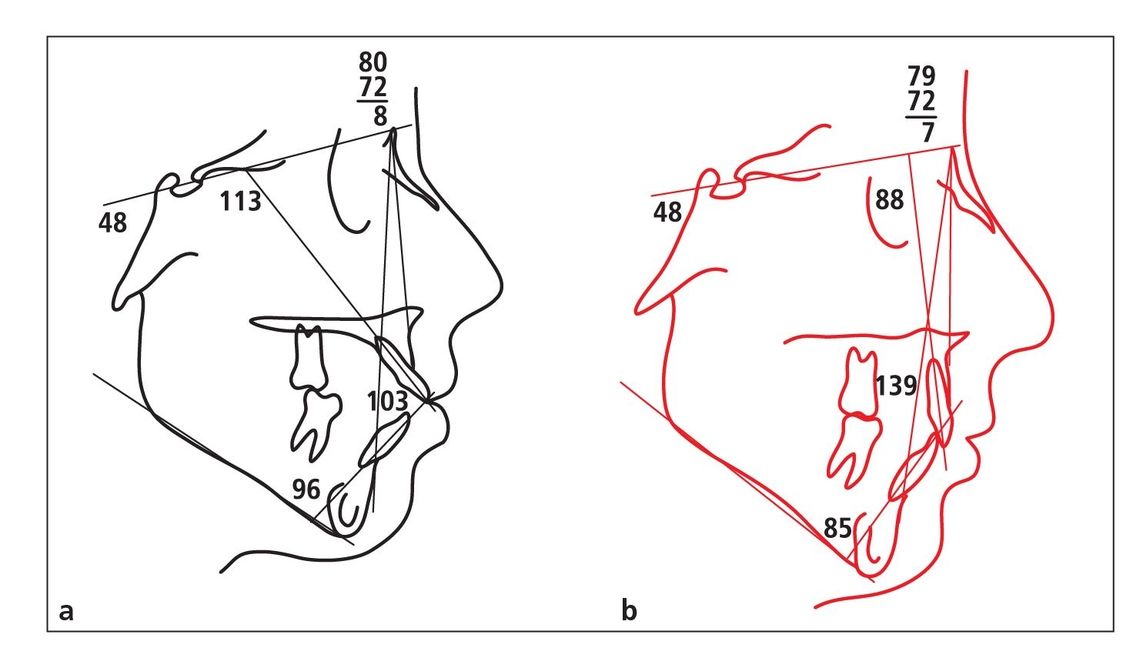
Fig 4-3 Patient with open bite. (a) Pretreatment cephalometric tracing. (b) Posttreatment cephalometric tracing. Notice the change in IMPA.
Exceptions
There are some exceptions to the 3-degree rule. For example, convex and concave profiles may require more changes. When convex profiles are treated with extractions, mandibular incisors will be uprighted much more than 3 degrees and will be very stable. In concave and deep bite cases, there is usually a need to advance the mandibular incisors more than 3 degrees to prevent a final concave profile. The stability in these cases is more suspect, so permanent retention is usually prescribed.
Regardless of the original position of the anterior teeth, the incisors will be close to the ideal position after placement of the 17 × 25 SS archwire. This is the case no matter if the patient has bimaxillary protrusion being treated with extraction or a Class II, Division 2 deep bite being treated without extraction. For example, the cephalometric tracings shown in Figs 4-2 and 4-3 demonstrate how the–5 degrees of torque respond in two different types of malocclusion.
Interincisal Angle
Although the final torque of the maxillary incisors has nothing to do with their original position, the original position of the mandibular incisors affects their final torque and is critical for long-term stability. Therefore, the interincisal angle is an important consideration. The interincisal angle is created by the relationship of the maxillary and mandibular incisors. Functionally, this angle affects anterior guidance, which is critical to healthy temporomandibular joints.
Esthetically, the lips “drape” the anterior teeth, so a balanced interincisal angle is necessary for a balanced soft tissue profile. The normal measurement for this angle is 130 to 135 degrees. If the anterior teeth are placed excessively forward, the profile will be protrusive and the lips will not touch when relaxed. Conversely, if the teeth are placed too far lingually, a concave profile will result. When discussing the interincisal angle, therefore, the decision to extract or not extract is critical to the final result.
Mechanics
Although I was taught to place torque in the archwire with 0.022 bracket slots to control each tooth, shortly after entering private practice, I changed to a 0.018 bracket slot with individual torques precut into each bracket. I found that I rarely needed to add or subtract torque in the archwire because the pretorqued appliance was working.
The same brackets respond differently to high-angle and low-angle patients. The only difference in the archwire is that opposite curves of Spee are placed in deep bite, low-angle cases and open bite, high-angle cases. The combination of change of torque in the archwire is caused by the curve placed in the wire and the different preexisting positions of the anterior teeth (upright in deep bite cases and flared in open bite cases). By creating accurate anterior torque control in both arches, an excellent interincisal angle is created.
0.018 versus 0.022
In volume 1 of this series, chapter 6 discusses the fundamental requirements for accurate torque control. For every 0.001 inch of “play” between the bracket slot and archwire size, 5 degrees of torque is lost.
To obtain the required torque for the incisors to create the best interincisal angle for the patient, it is necessary to understand the effective torque that is delivered by the various bracket prescriptions (Figs 4-4 and 4-5).
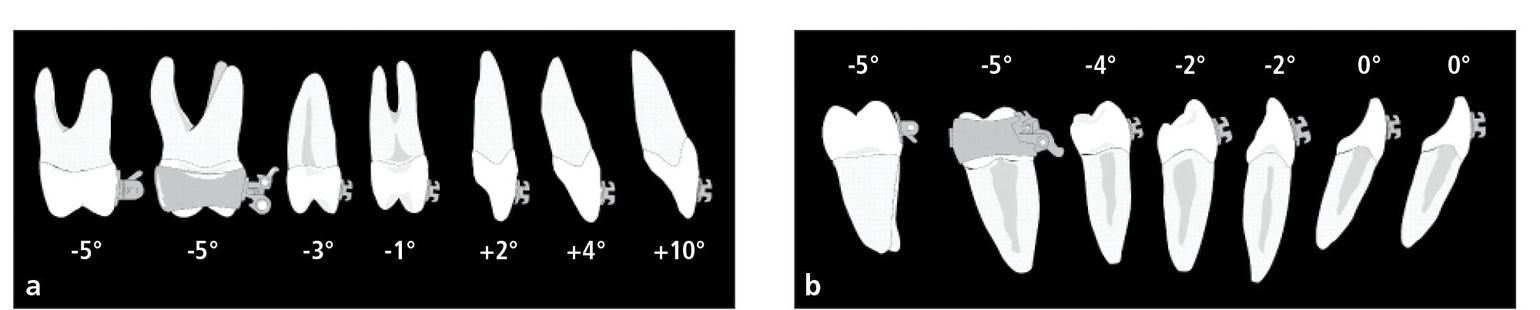
Fig 4-4 Effective bracket torques prescribed in the Alexander Discipline for 17 × 25 SS archwires. (a) Maxillary torque. (b) Mandibular torque.

Fig 4-5 Effective bracket torques prescribed in the Twin Bracket System for 0.022 slots. Fifteen degrees of torque are lost on each bracket. (a) Maxillary torque. (b) Mandibular torque.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


