CHAPTER 6
Transverse Skeletal Alteration
“Knowing is not enough; we must apply.”
—Leonardo da Vinci
Of the three skeletal dimensions, transverse dimensional changes are the most predictable. A narrow maxilla in a growing child can almost always be expanded with archwires or rapid palatal expansion (RPE) and have predictable and stable results. This can be considered a dentoalveolar or orthopedic correction. A narrow mandibular arch can then be expanded with controlled stability, usually with a lip bumper or other functional removable appliances. This is considered dentoalveolar expansion.
In nongrowing patients, nonsurgical palatal expansion is also possible, although done with more guarded expectations.
While achieving and maintaining skeletal correction in the sagittal and vertical dimensions is sometimes difficult to achieve and maintain, transverse correction and long-term stability can be much more successful if certain guidelines are followed.
This chapter focuses on three areas that must be addressed if we want long-term transverse correction: (1) mandibular intercanine width (3 × 3) (Fig 6-1), (2) maxillary intermolar width (6 × 6) (see Fig 6-1), and (3) maxillary and mandibular arch forms (Fig 6-2).
Mandibular Intercanine Width (3 × 3)
One of the goals of transverse control is to maintain the original mandibular intercanine width within 1 mm. This is true for extraction as well as nonextraction treatments. Again, Dr Tweed was right.
Some clinicians today will rationalize that in extraction cases, because the mandibular canines can be moved to a wider part of the arch in the extraction sites, the width between them can be expanded by more than 1 mm and remain stable. However, to my knowledge, there has never been any published long-term research that demonstrates permanent expansion of the mandibular intercanine width. I have never seen this situation in any extraction cases except where the canines have erupted lingually.
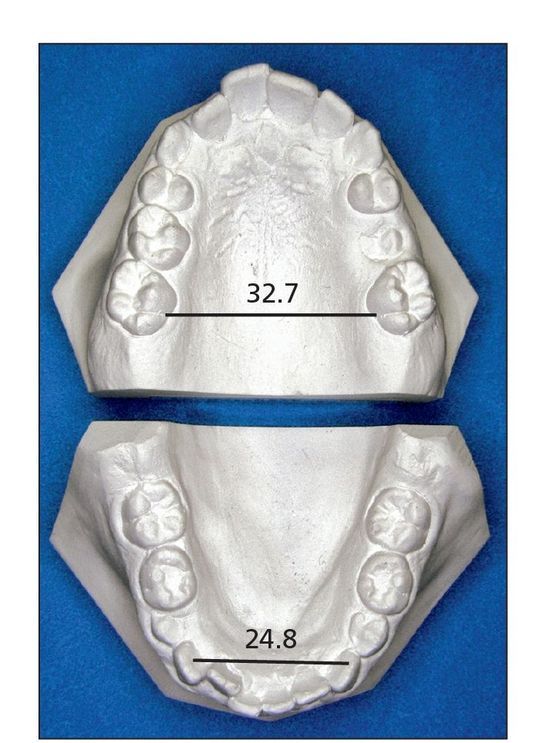
Fig 6-1 Mandibular arch with 3 × 3 measured and maxillary arch with 6 × 6 measured.
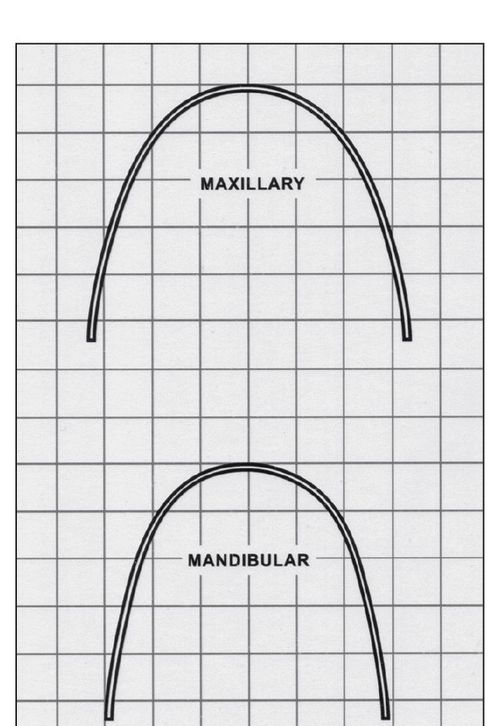
Fig 6-2 Template with maxillary and mandibular arch forms.
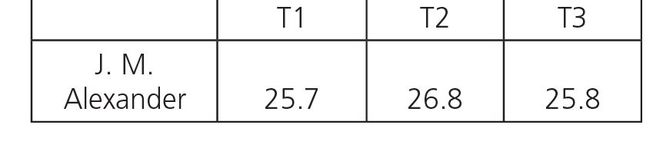
Table 6-1 Intercanine width after extraction (mm)
Evidence
Four long-term studies from the Room of Truth have substantiated this knowledge.1–4 Table 6-1 shows the long-term 3 × 3 measurements of J. M. Alexander’s study.3
Additionally, many other studies have been published with similar results. I would challenge any person who questions these conclusions to show significant long-term stability in patients with mandibular intercanine width expansion and no retention.
Mechanics
With some patients, controlling intercanine width can be just as difficult as controlling torque in mandibular incisors. Mandibular intercanine width can easily be expanded with a 0.016 nitinol (NiTi) archwire as crowded mandibular anterior teeth are unraveled. When a lip bumper is used, the intercanine width is also increased just by removing the pressure of the orbicularis oris muscles. However, this expansion will be temporary (Fig 6-3).
Final arch form is accomplished with the 17 × 25 stainless steel (SS) archwire. The original mandibular study model is used for a guide to shape the arch form of the six anterior teeth. The archwire should then be placed on top of the brackets in the patient’s mouth to check total arch form.
Maxillary Intermolar Width
Another goal of transverse dimension is to keep the maxillary intermolar width between 34 and 38 mm when measured from points created by the lingual marginal ridge of the maxillary first molars at the cervical line (Fig 6-5).
Evidence
The Ferris et al study published in 2005 evaluated long-term stability of RPE and lip bumper therapy followed by the use of fixed appliances4 (Fig 6-6). Of the 20 patients participating in the study (9 men and 11 women who had undergone initial treatment between the ages of 11 years 2 months and 13½ years), mean posttreatment time was 24 years, and mean time out of retention was 8 years.
Fig 6-3 Mandibular arch before (a) and after (b) lip bumper therapy.
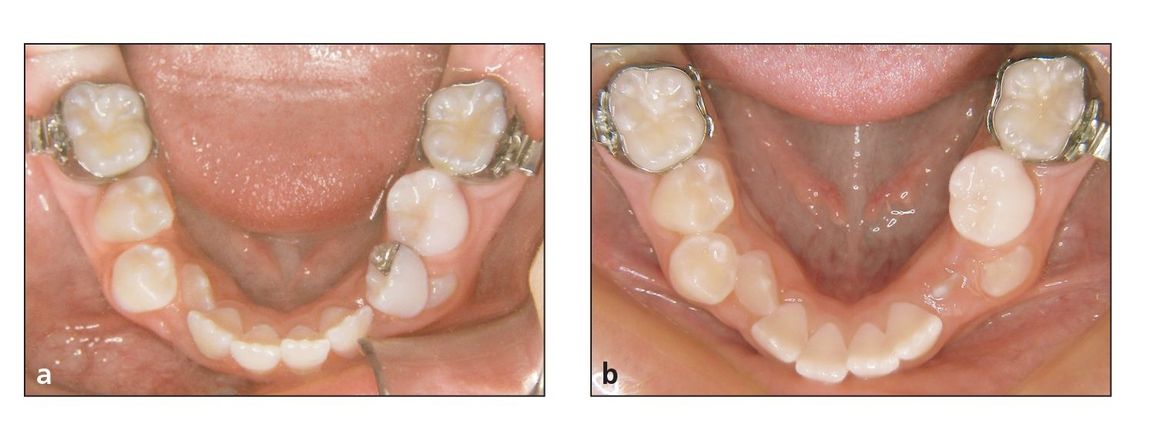
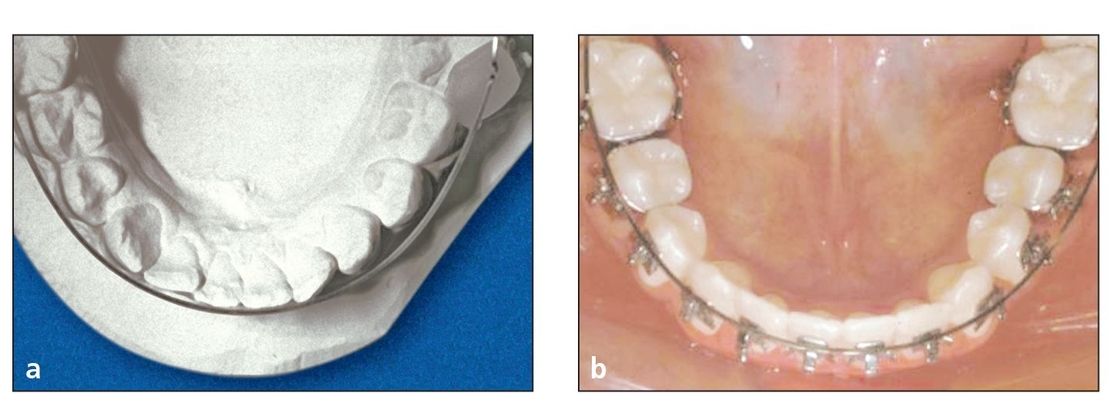
Fig 6-4 (a) Occlusal view of mandibular original study model with 3 × 3 measurements. (b) Occlusal view of patient while checking 3 × 3 width.

Fig 6-5 Caliper measuring maxillary 6 × 6.
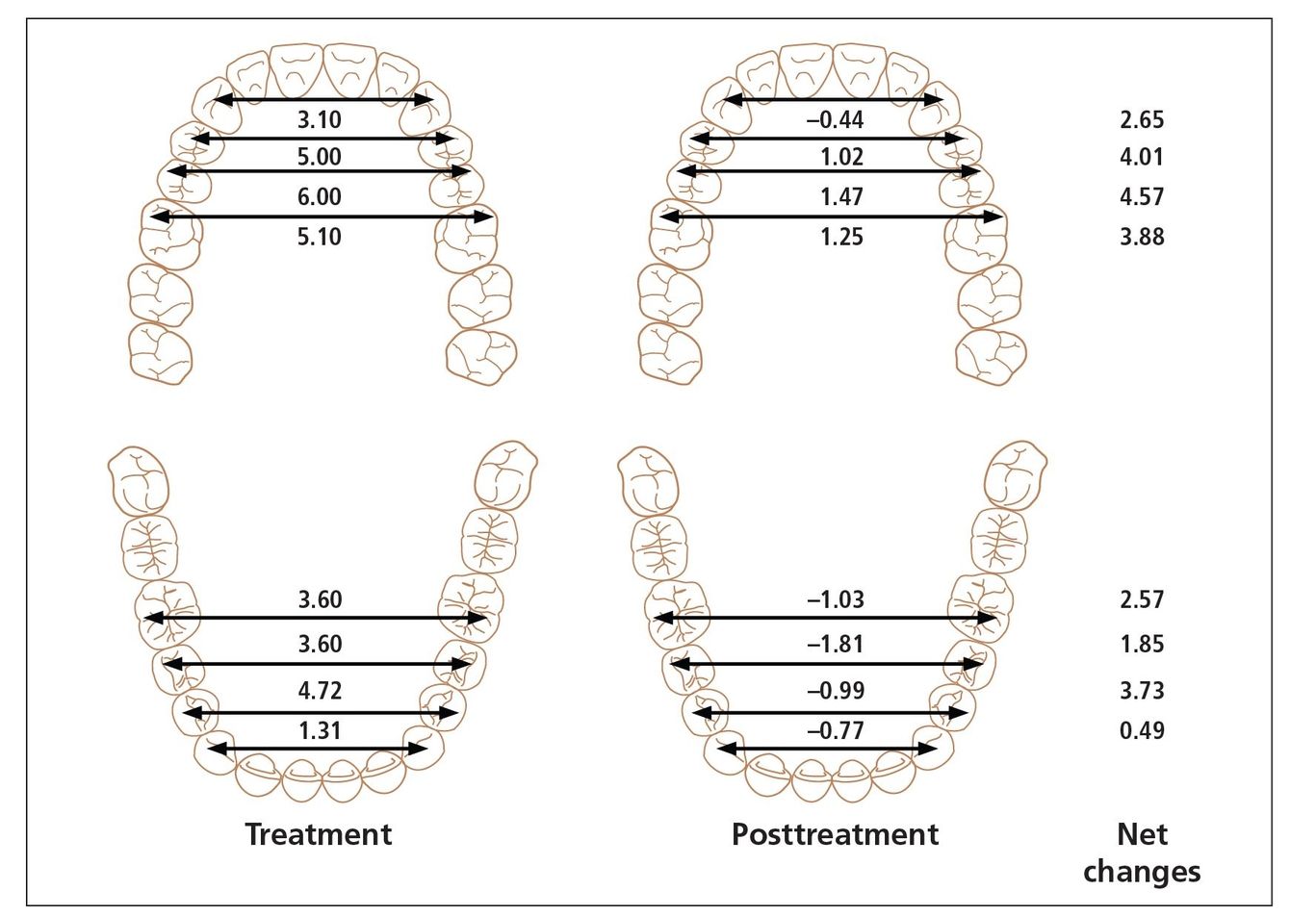
Fig 6-6 Ferris et al study: treatment and posttreatment (eight years postretention) changes in cusp-tip width of the maxillary and mandibular arches. The lateral measurements in this study were taken from cusp-tip widths rather than gingival margins, so the numbers may not coordinate with other studies.
The study concluded that RPE/lip bumper therapy followed by full fixed appliances significantly increases most arch dimensions and prevents expected decreases of other dimensions. There were long-term postretention decreases, but substantial net gains remained.
According to this study, therefore, RPE/lip bumper therapy followed by full fixed appliances is an acceptable way to treat patients with mild tooth size–arch length discrepancy (TSALD) in middle-late mixed to early permanent dentition. Mandibular intercanine width should be controlled rather than expanded whereas maxillary and mandibular interpremolar and intermolar widths can be expanded permanently.
Maxillary and Mandibular Arch Forms
The last important aspect of transverse control is the coordination of the mandibular intercanine width with the maxillary intermolar width, which creates the patient’s final arch form.
The final goal of transverse control is to avoid creating an arch form that is designed to fit a bracket system. Instead, we must look at the limitations of the positions of the teeth. After discussing the incisor mandibular plane angle (IMPA), intercanine width, and maxillary intermolar width, it makes sense that when we put these three measurements together, the arch form is automatically configured for us.
Mechanics
McKelvain’s study5 developed an arch form template (see Fig 6-2) that is used today on each of our patients. Although this arch form template fits the majority of our patients within one standard deviation, every archwire still must be individually adjusted for each patient.
Although the arch form must be designed within the confines of the mandibular 3 × 3 width and maxillary 6 × 6 width, each patient has his or her own best arch form.
Based on the many studies written inside the Room of Truth and the long-term stability of my patients, I have come to the following conclusions about ideal arch form:
- The anterior segment of any arch form should be dictated by the mandibular intercanine width (Fig 6-7) and the position of the mandibular incisors. Unless the canines have erupted abnormally lingually, the intercanine width should be expanded no more than 1 mm. In addition, the mandibular incisors should be kept in an upright position (Fig 6-8). This anterior segment of the mandibular arch form was taught by Tweed with the Bonwell-Hawley arch form.
- Because little variation in arch form can take place in the mandibular anterior segment, the maxillary anterior
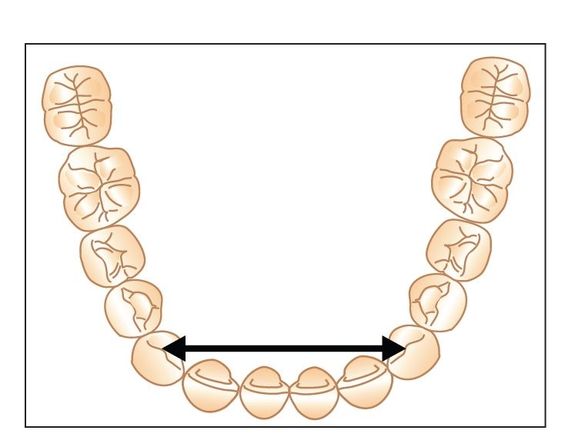
Fig 6-7 Final anterior arch form is partly dictated by the original intercanine width.
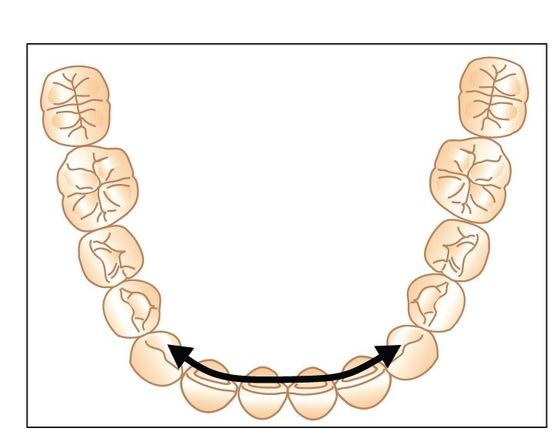
Fig 6-8 Final anterior arch form is also dictated by controlling the mandibular incisor position.
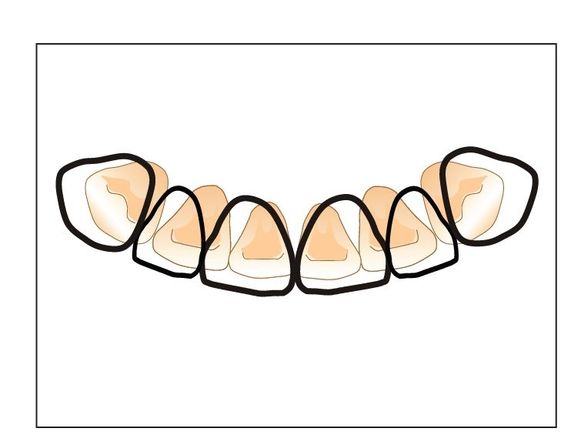
Fig 6-9 The arch form of the maxillary anterior teeth is dictated by the configuration of the mandibular canine-to-canine relationship.
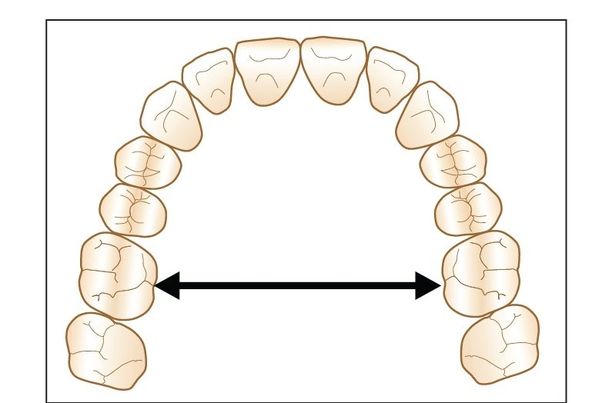
Fig 6-10 Maxillary intermolar width determines the final arch form. Using this technique to create the final arch form will always produce an ovoid shape.
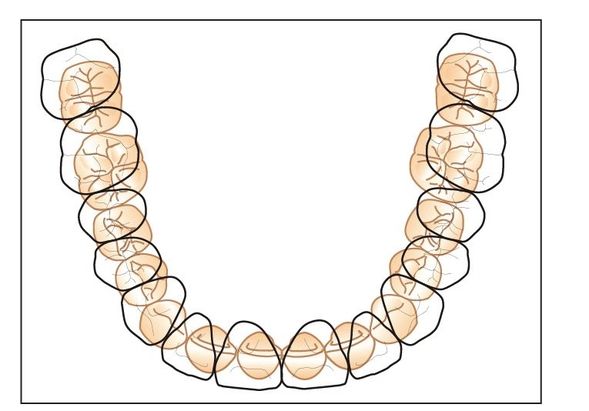
Fig 6-11 The mandibular posterior arch can then be expanded or constricted to occlude properly with the maxillary arch.
arch form, from canine to canine, must then conform to the mandibular arch form (Fig 6-9).
- The final shape of the posterior segments of the maxillary arch form is dictated by the maxillary intermolar width. Our studies have shown that the long-term posttreatment maxillary intermolar width after nonextraction therapy averages around 35 to 37 mm. This is measured at the lingual central groove of the maxillary first molars, at the cervical line (Fig 6-10). The posterior segments of the Alexander Discipline arch form are thus designed to conform to this width (Fig 6-11).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


