The Dynamics of Change
 Outline
OutlinePhysical Changes
Body
It is also a time when there is an increase in the mass of muscles, a redistribution of body fat, and an increase in the rate of skeletal growth. A growth spurt is associated with this time of life. This growth spurt follows two different forms, depending on gender. It appears earlier in females than in males. The average onset in males is 2 years later than that in females. The fact that males experience their growth spurt later than females and therefore have a longer maturation period before the growth period is one of the reasons why the height of males generally exceeds the height of females. The earlier growth spurt of females also accounts for the period of time during which mean height of a group of young female adolescents may exceed that of males. It is important to realize also that in females menarche serves as a signal that growth is ending, but for males no such marker exists. The magnitude of the velocity of change during the growth spurt also differs between the sexes. In 1975, Tanner and colleagues1 concluded that the growth spurt in females peaks at 9 cm change per year at age 12 years, and that in males it peaks at just over 10 cm at age 14 years.
Craniofacial Changes
During and following adolescence, continued changes in the skeletal growth of the face and skull take place because the facial sutures are still open and viable2 and mandibular growth can potentially continue. These changes not only cause variation and individuality in facial appearance3 but affect the dental structures as well. The continued changes make a final and unchanging dentition and occlusion a difficult concept to imagine, much less attain. There is a slow increase in facial height accompanied by an increase in prognathism in males.4,5
Profile changes occur as changes in specific locations take place. The brow area becomes larger as a result of pneumatization of the frontal sinuses and apposition on the glabella.6 Also, appositional changes during adolescence and early adult life in the frontal bone area and brow result in this area’s becoming more prominent.4 In adolescence the nose and chin also become more prominent. The tip of the nasal bone lies well ahead of the basal bone of the premaxilla. Soft tissue changes also contribute to the growth in the length of the nose and can affect the harmony existing between the nose, lips, and chin. The mandible shows a greater prognathism than the maxilla because of the circumpubertal growth spurt, which has more effect on the mandible than on the maxilla, especially in males. The chin also becomes more prominent owing to local bone deposition. Lip prominence is reduced by these changes in adjacent structures.
Underlying maxillary changes also occur. The maxillary sinuses, which have since birth expanded laterally and vertically, occupy the space left by the permanent teeth as they erupt. By puberty, the sinuses are usually fully developed, although they may continue to enlarge. There is considerable individual variation in the size of the maxillary sinuses, and they often lack symmetry. Lowering of the palatal vault continues because of remodeling. In 1966, Bjork7 concluded that sutural growth as well as appositional growth of the maxilla contributed significantly to the increase in the height of the maxillary body (Figure 36-1). This can be an example of sexual dimorphism in skeletal growth (Table 36-1). Vertical maxillary facial growth is often greater in females. Because the mandible does not continue to grow as much in females, marked vertical changes in the maxilla can result in downward and backward positioning of the mandible and an increase in facial convexity (Figure 36-2).4
 TABLE 36-1
TABLE 36-1
Growth of the Aging Skeleton: Sexual Dimorphism in Craniofacial Growth
| Females | Males | |
| Circumpubertal growth spurt | 10-12 years | 12-14 years |
| Mature size | Growth plateaus at age 14 years with increases to 16 years | Active growth to 18 years |
| Supraorbital ridges | Absent | Well developed |
| Frontal sinuses | Small | Large |
| Nose | Small | Large |
| Zygomatic prominences | Small | Large |
| Mandibular symphysis | Rounded | Prominent |
| Mandibular angle | Rounded | Prominent lipping |
| Occipital condyles | Small | Large |
| Mastoid processes | Small | Large |
| Occipital protuberance | Insignificant | Prominent |
From Behrents RG: Growth in the aging craniofacial skeleton, Ann Arbor, Mich, 1985, Center for Human Growth and Development, University of Michigan.
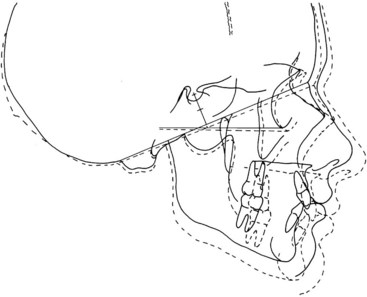
 FIGURE 36-1
FIGURE 36-1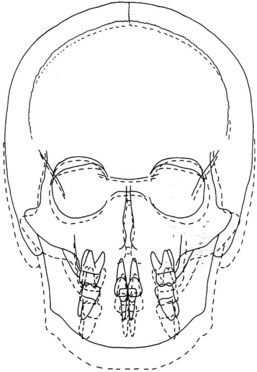
 FIGURE 36-2
FIGURE 36-2Mandibular growth contributes more than profile changes. This growth may be sufficient to provide room for the third molars. In many cases growth is inadequate, and these molars become impacted (Figure 36-3). The marked mesial inclination of the posterior permanent teeth diminishes somewhat as the mandible completes its growth from under the maxilla, and the lower incisors tend to become upright. Often this is accompanied by crowding of the lower incisors.2
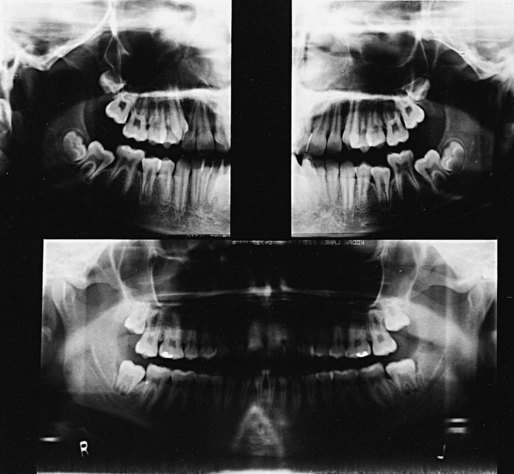
 FIGURE 36-3
FIGURE 36-3Late mandibular growth imparts an increase in the vertical height of the mandibular ramus, which becomes more upright. The elongation of the ramus accommodates the massive vertical expansion of the nasal region and the lowering of the palate, which is accompanied by dental eruption. Usually the maxillary and mandibular growths are compatible and coordinated. If they are not, significant orthodontic problems can result. Particularly in males, there can be late anterior growth that is undesirable.4
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


