Chapter 3
Treatment Planning and Managing Toothache
Aim
The aim of this chapter is to outline the principles of treatment planning. The management of the child with toothache will also be considered. The treatment of reversible and irreversible pulpitis will be compared and presented within the wider context of caries risk, the child’s potential for cooperation and the degree of parental support.
Outcome
On completing this chapter, the practitioner should feel confident in treatment planning and in the management of toothache in children and in the selection of the appropriate method of achieving pain control.
Introduction
Although dental caries is almost completely preventable, some parts of the UK have amongst the highest prevalence of the disease in Western Europe. The number of carious teeth that are treated by restoration is low, and this is particularly the case when primary teeth are considered. Indeed, the demand for general anaesthesia for removal of carious teeth is by far the most common reason for an out-patient paediatric hospital admission in many regions of the UK. The reasons for this are complex and relate to socio-economic status, ethnicity and geographic location. The solutions are equally complex and many are beyond the scope of the individual practitioner and therefore beyond the scope of this text. But how can the dental team manage a child with toothache?
Pragmatic treatment planning
Correct diagnosis is only the first part in the formulation of the treatment plan. The final piece of the treatment plan jigsaw is determined by measuring the likely compliance of the child and the level of parental support and consent. The best treatment plans are pragmatic – in other words, they will only be successful if they are achievable in the first place.
Dental treatment cannot be carried out without parental consent. This means that the parent or carer has a role in developing the definitive treatment plan. This is particularly true when the different treatment options (if there are any) are discussed. Therefore, the dentist has to explain the disease process to the patient and parent in a language they will understand. He/she also has to explain the management, and this is best achieved by demonstrating both the clinical and radiographic findings (Fig 3-1).
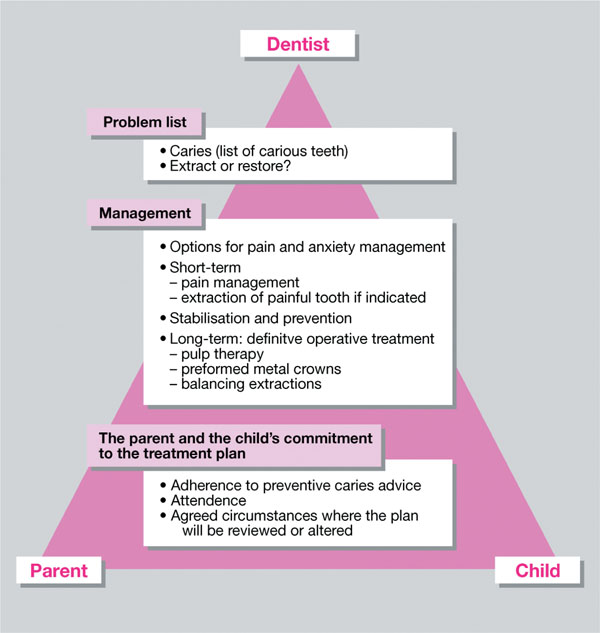
Fig 3-1 The conference between the dentist, child and parent is essential to success.
Problem List
A problem list can help focus the dentist’s attention on the important factors that determine the shape of the treatment plan. These factors include pain, caries risk, cooperation and the potential complexity of the operative treatment options.
The Stages of a Treatment Plan
A treatment plan is made up of a number of stages:
-
relief of pain
-
prevention at home
-
professional prevention
-
stabilisation of caries present
-
restorations
-
pulp therapy
-
extractions
-
behaviour management
-
reinforce prevention.
This system of planning care is based on putting prevention first after pain relief and is the focus of the treatment plan. Preventive treatments, particularly those provided by the patient and their family at home every day, will have the greatest long-term benefit on the patient’s oral health. There is also a hierarchy of treatment, commencing with simple, pleasant procedures, moving on as the patient’s confidence and compliance increases, to more technically demanding and perhaps more unpleasant ones.
Following extractions or other unpleasant procedures it is wise to end the course of treatment with a pleasant visit focusing on prevention. This will provide positive reinforcement and help erase unpleasant memories.
Analgesia, Sedation and General Anaesthesia
There is no doubt that restorations placed under local anaesthesia are superior in terms of quality and longevity. Unfortunately, not all children can cope with local anaesthetic injections at their initial presentation.
Depending on the child’s age, cooperation and the nature of the planned procedure, there may be a need for a decision on the appropriateness of sedation (usually inhalation sedation) or general anaesthesia to help the child cope with the required operative care. The choice to use either sedation or, particularly, general anaesthetia should always be made with a full assessment of the risks and benefits and consideration of any possible alternatives (Fig 3-2).
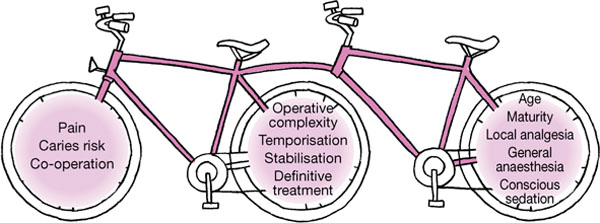
Fig 3-2 The final plan depends on the problem list and the expectation of how the child will cope to accept treatment.
The Child with Toothache
Diagnosis of toothache relies on a thorough history and examination. Even though this chapter focuses on toothache, the dentist must take care to exclude other causes of pain.
Common causes of oral pain in children include:
-
abscesses,
-
caries (often no pain),
-
trauma,
-
tooth wear,
-
infection,
-
soft tissue lesions (i.e. recurrent oral ulceration),
-
exfoliation/eruption.
Reversible or Irreversible Pulpitis?
The key to managing toothache, especially in primary teeth, is determining whether or not the pulpitis is reversible or irreversible. The correct diagnosis can be elicited through the history and the clinical and radiographic examination. A summary of this is shown in Table 3-1.
| Reversible Pulpitis | Irreversible Pulpitis/Abscess | |
| History |
|
|
| Examination |
|
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


