Chapter 5
Intracoronal Restorations for Posterior Primary Teeth
Aims
The aim of this chapter is to discuss the intracoronal restoration of carious primary teeth. In addition, the clinical relevance of the anatomical differences between the primary and permanent dentitions are highlighted.
Outcome
After reading this chapter, the practitioner should feel able to perform modern operative approaches to caries removal and intracoronal restoration of primary molar teeth and understand how these relate to the morphology of primary molars.
Introduction
Parents and dentists alike are keen to avoid the spectre of toothache in a child. Primary teeth have a key role to play in the future development of both occlusal development and in the acceptance of the child by their peers. The anatomical form of primary teeth, especially primary molars, means that caries can cause changes in the pulp faster than in permanent teeth. Fortunately the restorative techniques are simpler compared to permanent teeth and profit from primary tooth morphology.
Anatomy
The anatomical differences between primary and permanent teeth are illustrated in Fig 5-1. Compared to a permanent tooth, the anatomy of a primary tooth can be summarised as follows:
-
The enamel is thin, lighter in colour and easier to cut with a bur compared with enamel of permanent teeth.
-
The crown is bulbous, especially towards the cervical area.
-
There is a marked cervical constriction apical to the cervical bulge.
-
In molars, the occlusal table is narrow in a buccolingual direction.
-
The pulp horns extend high into the anatomical crown.
-
The enamel rods are inclined occlusally in the cervical region.
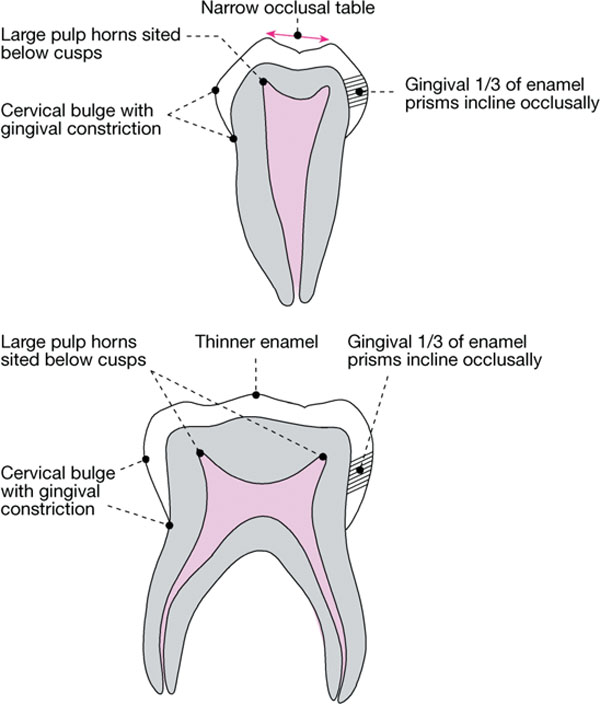
Fig 5-1 The anatomy of primary teeth.
Although the principles of caries removal in primary teeth are essentially the same as those for the permanent dentition, there are some differences that are important clinically. These are summarised in Table 5-1.
| Crown Morphology | Clinical Significance |
| Thinner enamel |
|
| Cervical bulge with gingival constriction |
|
| Narrow occlusal table |
|
| Broad contact areas located gingivally |
|
| Large pulp horns sited below cusps |
|
| Gingival third of enamel prisms incline occlusally |
|
Indications for Restoration
A minimal restoration, placed with relative ease when the lesion has just penetrated dentine and cavitated, can avoid the need for a larger restoration or even extraction later. In this way, dental operative procedures can be kept simple and used in combination with preventive care to ensure a positive attitude to dentistry and life-long oral health.
Primary teeth are restored in order to:
-
Prevent pain and sequelae, such as irreversible pulpitis and infection.
-
Avoid extraction in certain medical conditions (e.g. bleeding disorders).
-
Avoid extractions in anxious children.
-
Preserve masticatory function.
-
Maintain an intact arch (primary dentition).
-
Provide space maintenance (mixed dentition).
-
Maintain anterior aesthetics.
Sequential Planning
For most children, a period of acclimatisation is required before embarking upon a restorative approach. Remember to use language that is appropriate to the age of the child. In the very young, access for caries removal can be improved by the use of miniature burs in a miniature handpiece. If a child has experienced caries in the primary dentition, you should consider fissure sealing the first permanent molars upon eruption.
Cavity Preparation
In general, the same principles and approach apply to the preparation of primary teeth as for the permanent dentition, but there are several factors worthy of consideration when treating dental caries in primary teeth: moisture control, the longevity of restorative materials, the extent of the caries in relation to the pulp horns and the cooperation of the child.
Moisture Control
Ideally, this should be achieved using dental dam isolation, but lack of cooperation may lead to compromise. Good moisture control can be achieved using small saliva ejectors, cotton wool rolls and dry guards (Fig 5-2).
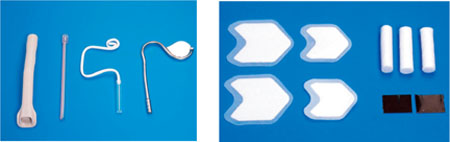
Fig 5-2 Equipment used to obtain moisture control (a) suction and saliva ejectors. (b) Cotton wool rolls and dry guards.
Choice of Material and Durability of Restorations
When placing a restoration in a primary tooth the dentist has to decide whether the filling is to last the lifetime of the tooth or if it is a temporary restoration that she/he expects to eventually replace. This choice is dependent on various factors, not least the expected longevity of the tooth. Nevertheless, in terms of durability the selection of materials can be summarised as follows:
-
Plastic restorations, such as amalgam, composite resins and glass ionomer cements perform best in one or two surface restorations. The glass ionomer materials have the advantage of directly adhering to tooth structure. They also release fluoride, although the clinical significance of this is unproven.
-
The newer resin-modified glass ionomer cements and compomers have the advantage of directly adhering to tooth tissue and a command set due to the resin component. This may be helpful when dealing with a wriggly child.
-
The more recent resin-modified glass ionomers and viscous glass ionomers have the advantages of glass ionomer but with improved strength.
-
The compomers appear to have survival rates similar to amalgam in class II cavities and have the advantage of adhering to tooth tissue via bonding agents.
-
The recommended restoration for primary molars with two or more carious surfaces is the preformed metal crown (stainless steel crown), and these restorations outperform other materials in all but the smallest of single surface restorations.
Two main factors affect the choice of material – those relating to the tooth to be restored and factors pertinent to the patient.
Tooth factors
-
The extent of the carious lesion (linked with durability).
-
The cavity shape after caries removal (e.g. method of retention, maintaining healthy tooth tissue).
Patient factors
-
Efficacy of isolation and moisture control (moisture-sensitive techniques).
-
Caries rate (temporise initially to obtain caries control).
-
Aesthetic expectations.
Caries in Primary Posterior Teeth
These can be put into the following subcategories:
-
Pit and fissure caries.
-
Approximal caries with pit and fissure caries.
-
Approximal caries without pit and fissure caries.
Useful Instruments for Caries Removal
-
Small sharp excavators.
-
Slow speed: round and flat fissure steel burs.
-
High speed: small round and straight diamond burs.
Pit and Fissure Caries
Occlusal pit and fissure caries removal is shown in Fig 5-3.
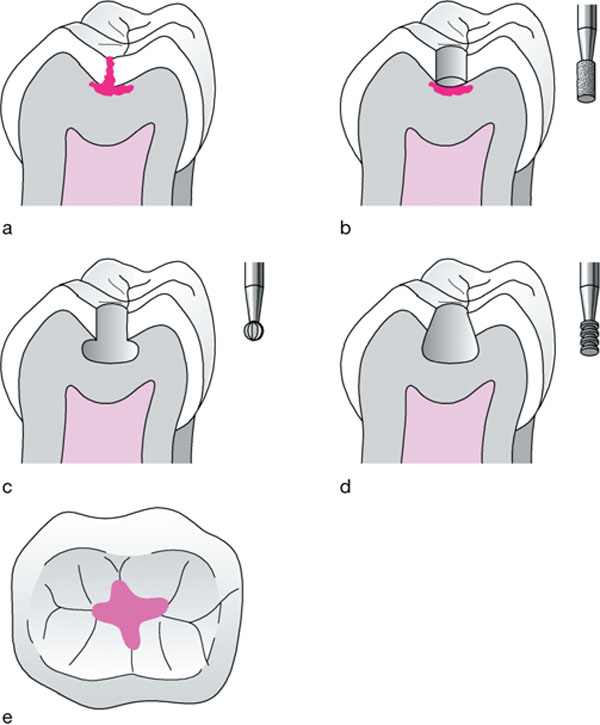
Fig 5-3 Occlusal pit and fissure caries removal. (a) Occlusal caries into dentine. (b) Access through carious enamel to carious dentine via straight diamond or steel flat fissure bur. (c) Caries removal leaving unsupported enamel, which should be removed. (d) Outline of cavity with a flat, slightly concave floor and walls diverging from the occlusal to provide retention for amalgam. (e) Outline is smooth without sharp angles and extends to include carious tissue only.
Access
-
Penetrate the occlusal surface within the carious area just into dentine (to a depth of 1.5mm x 0.5mm into d/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


