The Dynamics of Change
 Outline
OutlinePhysical Changes
Body
The median (50th percentile) weight and height of 6-year-old boys in the United States are 47.5 pounds and 45.5 inches, whereas the same medians for girls are 46 pounds and 45 inches. By the time children reach age 12 years, boys will be 90 pounds and 59 inches, and girls will be 90.25 pounds and 59.5 inches. This is a time of substantial continuous growth.1
Craniofacial Changes
The period from age 6 through 12 years represent a continuous progression of the growth in the head and neck. From age 5 to 10 years (approximately the age range of interest here), neural and cranial growth are found to be almost entirely complete (Figure 29-1). During this same age span, the jaws (maxilla = A = 2 and mandible = B = 3 of Figure 29-1) grow at a faster rate than the cranium.
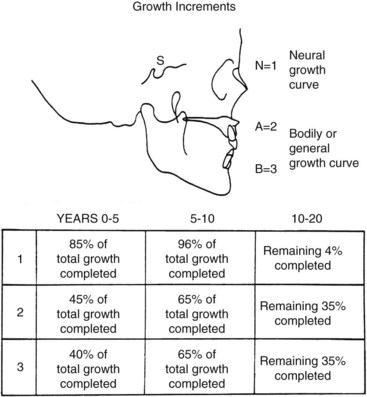
 FIGURE 29-1
FIGURE 29-1Using the Bolton standards for illustrative purposes,2 nasal projection and increased mandibular prominence are demonstrated (Figure 29-2). The nasal cartilage and mandibular condyle continue to grow by endochondral bone formation for some time, although the female mandibular growth spurt is most likely completed during this time period, and the male’s is yet to come. Growth modification can therefore be performed in this age group. Changes in cranial base length caused by endochondral bone formation at the sphenooccipital synchondrosis cease in early adolescence, but some appositional changes continue to occur at the basion and nasion. Vertically, there is a continued lowering of the palatal vault with sutural growth and apposition on the oral side of the palate and resorption on the nasal side as the intramembranous process of bone formation continues. Vertical facial growth is also complemented by dentoalveolar growth as the permanent teeth erupt and the alveolar ridges develop.
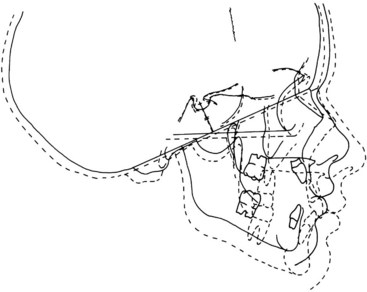
 FIGURE 29-2
FIGURE 29-2In the transverse plane, there is continued growth at the midpalatal suture. Most transverse palatal sutural growth in completed for females during this period when the first bridging of the suture occurs. Transverse appositional widening of the alveolar ridge occurs with eruption of the permanent teeth. Widening of the anterior arch accompanies lateral incisor eruption and is followed by width increases in the canines and premolars (Figure 29-3).
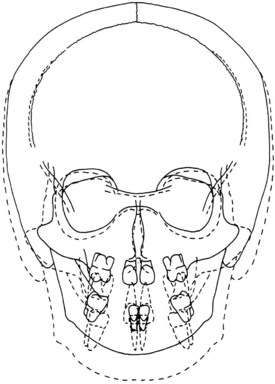
 FIGURE 29-3
FIGURE 29-3Dental Changes
Early during this period of time, many children experience the eruption of all four first permanent molars and the exfoliation of the mandibular and maxillary primary central and lateral incisors with a subsequent eruption of permanent incisors between the ages of 6 and 7 years (see Table 12-5). The maxillary permanent lateral incisors may erupt later than age 7 years in some children. The eruption of the anterior teeth should be carefully and easily observed by the practitioner for developmental and esthetic reasons.
With the exception of the third molars, all of the permanent teeth usually have erupted by the end of the twelfth year, and the enamel of all of the permanent teeth is complete by age 8 years. In the mandibular arch and following the first permanent molars and central incisors, the teeth erupt in immediate succession, that is, centrals, laterals, canines, first and second premolars, and second permanent molars from 6 to 7 years through 11 to 13 years of age. The same sequence takes place in the maxillary arch except for the maxillary canine, which usually erupts after the one or both premolars and at about the same time as or before the eruption of the second permanent molars (Figure 29-4).
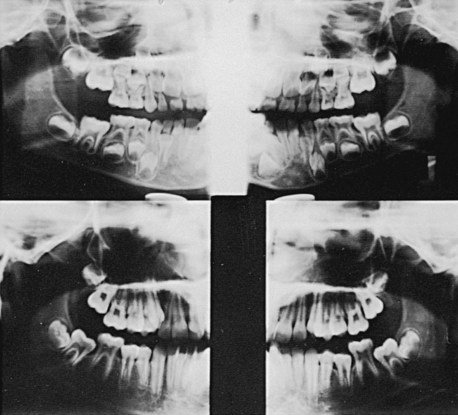
 FIGURE 29-4
FIGURE 29-4The mandibular central incisor roots are complete by age 9 or 10 years. The roots of the four first permanent molars, the maxillary central incisors, and the mandibular lateral incisors are usually complete by age 10 years. The roots of the maxillary lateral incisors are complete by age 11 years.3
Because the position of the dental lamina of the permanent teeth is located to the lingual of all of the primary teeth (except for the dental lamina coming off the second primary for the three permanent molars), the anterior teeth develop in their vault or crypt lingual to and near the apex of the primary incisors. When the roots begin to form on the permanent teeth, they start to migrate to the oral cavity. Generally, they follow a pattern such that they come across the primary root, resorbing it and erupting slightly lingual to the location sustained by the primary tooth (Figure 29-5). Ultimately, the permanent teeth are usually angulated more buccally compared with their primary predecessors (Figure 29-6). The developing premolars develop between the roots of the primary molars and continue to erupt in a slightly buccal position.
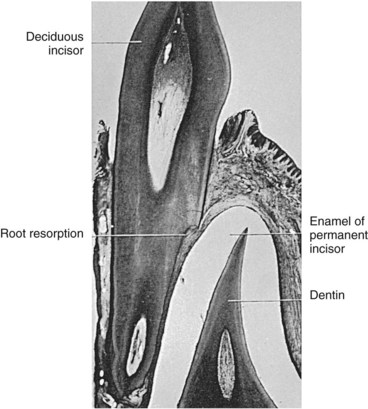
 FIGURE 29-5
FIGURE 29-5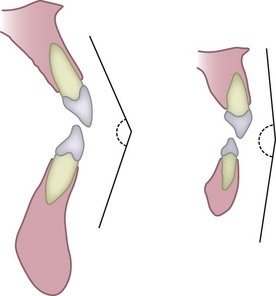
 FIGURE 29-6
FIGURE 29-6It is normal to find diastemas between the primary incisors. This helps provide space for the larger permanent incisors. The permanent canine in the maxillary arch is usually the last permanent tooth to erupt mesial to the first permanent molar. As the permanent canine begins to erupt, it migrates down the distal root surface of the maxillary lateral incisor and ultimately moves the crowns of the incisors mesially and will close moderate to small diastemas. This period of development has been called the “ugly duckling stage” (Figure 29-7).4
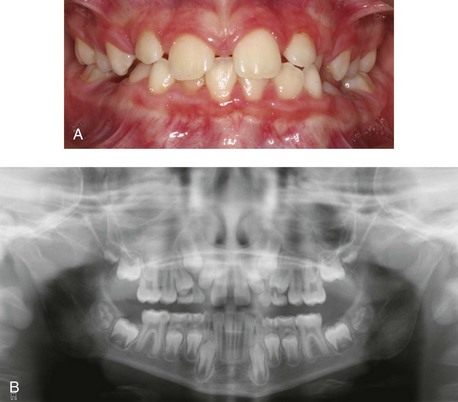
 FIGURE 29-7
FIGURE 29-7Cognitive Changes
According to Piaget,5 the ages between 6 and 12 years roughly approximate the third major developmental stage of cognition, that is, the phase of concrete operations. Piaget proposed the following four major periods of intellectual development:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


