Chapter 29
Psychiatric Disorders
Mental disorders are common in today’s society. Approximately one third of the population in the United States will have at least one psychiatric disorder during their lifetime, and 20% to 30% of adults in the United States will experience one or more psychiatric disorders during a 1-year period. About 5% of the population suffers from serious affective or mood disorders. Schizophrenic disorders are reported in 1.1%.< ?xml:namespace prefix = "mbp" />
Psychiatric problems, which can affect the clinical course in various medical illnesses, increase required duration of treatment, decrease the patient’s functional level, and have a negative impact on overall prognosis and outcome. Disorders related to drug and alcohol use account for a significant proportion of the treatment-related psychiatric issues. In the elderly population, a high prevalence of psychiatric complications is associated with medical illness. About 11% to 15% of these patients experience depressive symptoms, and between 10% and 20% have anxiety disorders, including phobias. Phobia is the most common psychiatric disorder in women older than 65 years of age. Approximately 20% of elderly persons have a substance abuse disorder.
This chapter provides an overview of mood disorders, somatoform disorders, and schizophrenia, with an emphasis on drugs used to treat these conditions and their significant adverse reactions and interactions with drugs used in dentistry. Also discussed are specific considerations in the dental management of patients with these disorders.
Mood Disorders
Definition
Mood disorders represent a heterogeneous group of mental disorders that are characterized by extreme exaggeration and disturbance of mood and affect. These disorders are associated with physiologic, cognitive, and psychomotor dysfunction. Mood disorders, which tend to be cyclic, include depression and bipolar disorder.
Epidemiology
Incidence and Prevalence
About 5% of the adults in the United States have a significant mood disorder. Mood disorders are more common among women (
TABLE 29-1 Epidemiology of Mood Disorders
| Variable | Depressive Disorders | Bipolar Disorders |
|---|---|---|
| Prevalence |
|
|
| Age at onset | ||
| Family and genetic studies | Bipolar patients have many relatives with bipolar disorder, cyclothymia, unipolar depression, and schizoaffective disorder | |
| Twin studies | 72% concordance in monozygotic twins, 19% in same sex dizygotic twins |
Data from Schiffer RB: Psychiatric disorders in medical practice. In Goldman L, Ausiello D, editors: Cecil textbook of medicine, ed 23, Philadelphia, Saunders, 2008; and Kahn DA: Mood disorders. In Cutler JL, Marcus ER: Saunders text and review: psychiatry, Philadelphia, Saunders, 1999.
The prevalence of major depression is fairly consistent across races and cultures. However, this disorder occurs with greater frequency among recent immigrants and the displaced.
The lifetime prevalence of dysthymia, a chronic, milder form of depression, is 2.2% in women and 4.1% in men.
Etiology
Several theories have been presented to explain the origin of mood disorders. Reduced brain concentrations of norepinephrine and serotonin (neurotransmitters) for some time have been believed to cause depression. Increased levels of these neurotransmitters have contributed to the onset of mania. The causes of depression and mania now appear to be complex.
Evidence for a genetic predisposition to bipolar disorder is significant. The concordance rate for monozygotic twin pairs approaches 80%, and segregation analyses are consistent with autosomal dominant transmission. Multiple genes are likely to be involved, with strongest evidence for loci on chromosomal arms 18p, 18q, 4p, 4q, 5q, 8p, and 21q.
Positron emission tomography (PET) studies show decreased metabolic activity in the caudate nuclei and frontal lobes in depressed patients that returns to normal with recovery. Single-photon emission computed tomography (SPECT) studies show comparable changes in blood flow.
Psychosocial theory focuses on loss as the cause of depression in vulnerable persons. Mania receives much less attention because it is thought to be more of a biologically caused disorder.
Clinical Presentation and Medical Management
Depressive Disorders
The Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR), lists three types of depressive disorders: major depression, dysthymic disorder, and depression not otherwise specified (NOS).

Box 29-1 Diagnostic Criteria for Depressive Disorders
From Schiffer RB: Psychiatric disorders in medical practice. In Goldman L, Ausiello D, editors: Cecil textbook of medicine, ed 23, Philadelphia, 2008, Saunders.

Bipolar Disorder
The DSM-IV lists four types of bipolar disorder: bipolar I, bipolar II, cyclothymic, and bipolar disorder NOS (
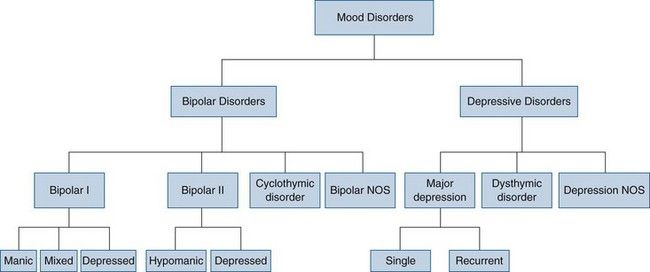
FIGURE 29-1 Mood disorders listed in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV-TR). Patients with bipolar disorder have had at least one episode of mania or hypomania. Cyclothymic disorder consists of recurrent brief episodes of hypomania and mild depression. Major depression usually is recurrent but sometimes happens as a single lifetime episode. Dysthymic disorder is mild depression that lasts at least 2 years.
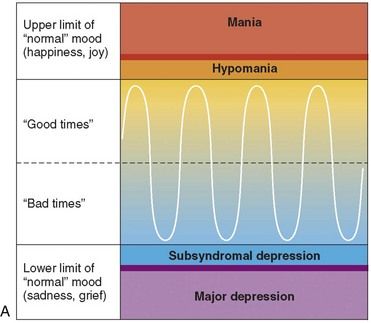
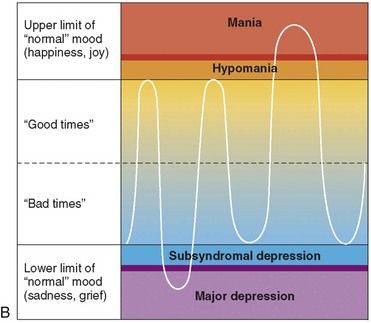
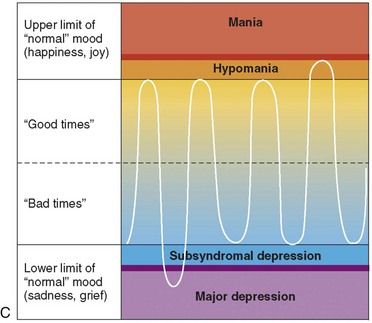
FIGURE 29-2 A, Normal mood cycles. B, Bipolar type I disorder. C, Bipolar type II disorder.
(From Khalife S: Bipolar disorder. In Carey WD, et al, editors: Current clinical medicine 2009—Cleveland Clinic, ed 2, Philadelphia, 2010, Saunders.)
TABLE 29-2 Clinical Features of Hypomania and Mania
| Feature | Hypomania | Mania |
|---|---|---|
| Appearance | May be unremarkable Demeanor may be cheerful |
Often striking Clothes may reflect mood state Demeanor may be cheerful Disordered and fatigued in severe states |
| Behavior | Increased sociability and loss of inhibition | Overactivity and excitement Social loss of inhibition |
| Speech | May be talkative | Often pressured, with flight of ideas |
| Mild elation or irritability | Elated or irritable Boundless optimism Typically, no diurnal pattern May be labile |
|
| Vegetative signs | Increased appetite Reduced need for sleep Increased libido |
Increased appetite Reduced need for sleep Increased libido |
| Psychotic symptoms | Not present | Thoughts may have an expansive quality |
| Thoughts may have an expansive quality | Delusions and second-person auditory hallucinations may be present, often grandiose in nature Schneiderian First Rank (symptoms associated with schizophrenia) symptoms found in 10-20% |
|
| Cognition | Mild distractibility | Marked distractibility More marked disturbances in severe states |
| Insight | Usually preserved | Insight often lost, especially in severe states |
From Mackin P, Young A; Bipolar disorders. In Wright P, Stern J, Phelan M, editors: Core psychiatry, ed 2, Edinburgh, 2005, Elsevier.
Bipolar II disorder (see
The diagnosis of bipolar disorder is made as soon as the patient has one manic episode, even if that person has never had a depressive episode. Most patients who become manic will eventually experience depression. However, about 10% of patients in whom bipolar disorder is diagnosed appear to have only manic episodes.
Men tend to have a greater number of manic episodes and women, more numerous depressive episodes. Untreated patients with bipolar disorder will experience a mean of nine affective episodes during their lifetime. The length of each cycle tends to decrease, although the number of cycles increases with age (
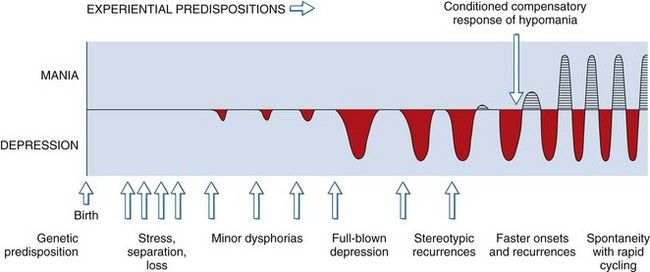
FIGURE 29-3 Natural history of recurrent mood disorders: an integrated model. Genetic factors and early environmental stress may predispose to development of a mood disorder. Early episodes are likely to be precipitated by environmental stress; later episodes are more likely to occur closer together and spontaneously, without precipitants.
Treatment of Mood Disorders
TABLE 29-3 Commonly Used Antidepressants (by Structural Group)
| Drug | Trade Name | Comments |
|---|---|---|
| Tricyclic | ||
| Amitriptyline | Elavil | |
| Trimipramine | Surmontil | |
| Desipramine | Norpramin | |
| Doxepin | Sinequan | |
| Imipramine | Tofranil | |
| Nortriptyline | Pamelor | |
| Protriptyline | Vivactil | |
| Tetracyclic | ||
| Maprotiline | Ludiomil | |
| Selective Serotonin Re-uptake Inhibitors | ||
| Escitalopram | Lexapro | |
| Fluoxetine | Prozac | |
| Fluvoxamine | Luvox | |
| Paroxetine | Paxil | |
| Sertraline | Zoloft | |
| MAOIs | Patients taking these drugs must be on a tyramine-free diet. | |
| Phenelzine | Nardil | |
| Tranylcypromine | Parnate | |
| Atypical or Nontricyclic | ||
| Nefazodone | Serzone | As effective as imipramine |
| Venlafaxine | Effexor | SNRI; may be effective in treatment of resistant depression |
| Amoxapine | Asendin | |
| Bupropion | Wellbutrin | May be especially helpful for atypical depression |
| Mirtazapine | Remeron | Increase at 1- to 2-week intervals. |
| Trazodone | Desyrel | Helpful as a second drug for sleep disturbance |
| Duloxetine | Cymbalta | Additionally useful in pain syndromes |
MAOIs, Monoamine oxidase inhibitors; SNRI, Serotonin-norepinephrine reuptake inhibitor.
Data from Schiffer RB: Psychiatric disorders in medical practice. In Goldman L, Ausiello D, editors: Cecil textbook of medicine, ed 23, Philadelphia, 2008, Saunders.
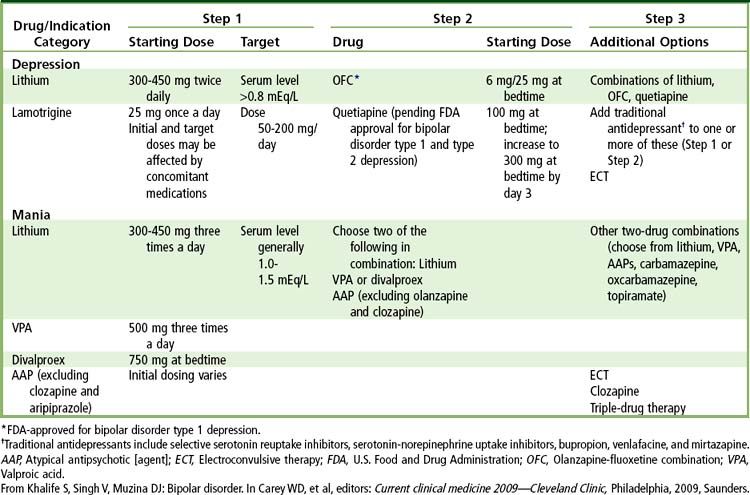
The mainstays of drug therapy for bipolar disorders are the mood-stabilizing drugs, which generally act on both mania and depression (
Mixed depressive and manic episodes are difficult to manage. First the manic behavior needs to be stabilized, and then the depression is addressed. An atypical antipsychotic (olanzapine) or a mood stabilizer is administered to stabilize the manic behavior, and depression is addressed with a standard antidepressant drug (fluoxetine). Another approach is to use a mood stabilizer and a combination agent consisting of an antidepressant plus an atypical antipsychotic—the olanzapine-fluoxetine combination (OFC) drug available as Symbyax.
Electroconvulsive therapy is an effective antimanic treatment.
It takes about 7 to 10 days for lithium to reach full therapeutic effectiveness. With most antidepressant drugs, a delay (10 to 21 days) is noted before full therapeutic benefits are achieved.
Patients who have had two or three episodes of bipolar disorder, including depressive episodes, usually are treated indefinitely because of the near certainty of relapse. Lithium is the treatment of choice. About one third of patients will not experience additional episodes and are considered cured; a third of those who take lithium will experience less frequent or less severe episodes and will function well; and the remaining third of patients will continue to have frequent and severe episodes with ongoing disability.
An estimated 30,000 suicides occur each year in the United States. About 70% of these involve persons with major depression. The physician must consider suicidal lethality in the management of patients with depression. In general, the risk for suicide is increased in association with the following factors: alcoholism, drug abuse, social isolation, elderly male status, terminal illness, and undiagnosed or untreated mental disorders. Patients at greatest risk are those with a history of previous suicide attempts, drug or alcohol abuse, recent diagnosis of a serious condition, loss of a loved one, or recent retirement, and those who live alone or lack adequate social support. Persons with a suicide plan and the means to carry out that plan are at greatest risk for suicide. Once medical control is attained in the patient with a mood disorder, insight-oriented psychotherapy often is initiated as an adjunct for management of the patient’s condition.
Somatoform Disorders
Definition
Persons with somatoform disorders have physical complaints for which no general medical cause is present. Associated unconscious psychological factors contribute to the onset, exacerbation, or maintenance of physical symptoms. The following conditions are regarded as somatoform disorders: somatization, conversion disorder, pain disorder, and hypochondriasis (
TABLE 29-5 Somatoform Disorders
| Somatoform Disorder | Features |
|---|---|
| Somatization disorder | Chronic multisystem disorder characterized by complaints of pain, and gastrointestinal and sexual dysfunction. Onset usually is early in life, and psychosocial and vocational achievements are limited. |
| Rarely affects men. Diagnostic criteria include four pain symptoms plus two gastrointestinal symptoms, plus one sexual-reproductive symptom, plus one pseudoneurologic symptom. | |
| Conversion disorder | Syndrome of symptoms or deficits mimicking neurologic or medical illness in which psychological factors are judged to be of etiologic importance. Patients report isolated symptoms that have no physical cause (blindness, deafness, stocking anesthesia) and that do not conform to known anatomic pathways or physiologic mechanisms. In a group of such patients followed over time, a physical disease process will become apparent in 10% to 50%. |
| Pain disorder | Clinical syndrome characterized predominantly by pain in which psychological factors are judged to be of etiologic importance |
| Hypochondriasis | Chronic preoccupation with the idea of having serious disease. This preoccupation usually is poorly amenable to reassurance. |
| May consist of a morbid preoccupation with physical symptoms or bodily functions. Can be described as “illness is a way of life.” | |
| Body dysmorphic disorder | Preoccupation with an imagined or exaggerated defect in physical appearance |
| Other somatoform-like disorders | |
| Factitious disorder | Intentional production or feigning of physical or psychological signs when external reinforcers (e.g., avoidance of responsibility, financial gain) are not clearly present |
| Voluntary production of symptoms without external incentive | |
| More common in men and seen in health care workers more often | |
| Skin lesions more common than oral (oral lesions cannot be seen) | |
| Oral lesions include those associated with self-extraction of teeth, picking at the gingiva with fingernails, nail file gingival injury, and application of caustic substances to the lips. | |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


