Oral Habits
 Outline
OutlineIf no dental changes have occurred, no treatment can be advocated on the grounds of dental health, but some patients and parents may want treatment because digit or pacifier habits become less socially acceptable as the child becomes older. One study has shown that school-aged children consider thumb suckers significantly less intelligent, less attractive, and less desirable as friends.8 Efforts to discourage the habit may involve as little as a conversation between the dentist and the child, or they may involve more complex appliance therapy. The most important point to remember about any intervention is that the child must want to discontinue the habit for treatment to be successful.
Thumb and Finger Habits
Thumb and finger habits make up the majority of oral habits. About two thirds of such habits are ended by 5 years of age.14 Dentists are often questioned about the kinds of problems these habits may cause if they are prolonged. The malocclusions caused by nonnutritive sucking may be more of an individual response than a highly specific cause-and-effect relationship.4 The types of dental changes that a digit habit may cause vary with the amount of force applied to the teeth and how long the force is applied (daily and in months or years) as well as the manner in which the digit is positioned in the mouth. Research and clinical experience have shown that as little as 35 grams of force can tip a tooth.26 It is apparent that children vary in the amount of force applied during sucking. Some suck with a great deal of intensity and others essentially rest the digit in their mouth. The amount of time spent sucking a digit will have an impact on tooth movement. The amount of time sucking (in months) probably plays the most critical role in tooth movement caused by a digit habit.24 Clinical experience suggests that 4 to 6 hours of force per day is probably the minimum necessary to cause tooth movement.26 Therefore a child who sucks intermittently with high force may not produce much tooth movement at all, whereas a child who sucks with less force but continuously (for more than 6 hours) can cause significant dental change, which is consistent with the equilibrium theory. The duration of digit sucking habits (months or years) is positively related to an increased prevalence of anterior open bite or reduced overbite, increased overjet, greater maxillary arch depth, and decreased maxillary arch width.24 The most frequently reported dental signs of an active habit are the following:
2. Facial position of the upper incisors and lingual position of the lower incisors leading to increased overjet
Anterior open bite, or the lack of vertical overlap of the upper and lower incisors when the posterior teeth are in occlusion, develops because the digit rests directly on the incisors (Figure 26-1). This prevents complete or continued eruption of the incisors, whereas the posterior teeth are free to erupt. Anterior open bite may also be caused by intrusion of the incisors. However, inhibition of eruption is easier to accomplish than true intrusion, which would be the result of a habit of greater duration.

 FIGURE 26-1
FIGURE 26-1Faciolingual movement of the incisors depends on how the thumb or finger is placed and how many fingers are placed in the mouth. Some consider this positional variable to be a confounding factor related to force and duration of the habit. Usually, the thumb is placed so that it exerts pressure on the lingual surfaces of the maxillary incisors and on the labial surfaces of the mandibular incisors (Figure 26-2). A child who actively sucks can create enough force to tip the upper incisors facially and the lower incisors lingually. The result is an increased overjet and, by virtue of the tipping, decreased overbite.
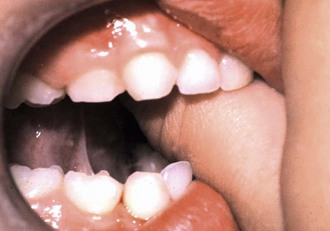
 FIGURE 26-2
FIGURE 26-2Maxillary arch constriction is probably due to the change in equilibrium balance between the oral musculature and the tongue.27 When the thumb is placed in the mouth, the tongue is forced down and away from the palate. The orbicularis oris and buccinator muscles continue to exert a force on the buccal surfaces of the maxillary dentition, especially when these muscles are contracted during sucking. Because the tongue no longer exerts a counterbalancing force from the lingual surface, the posterior maxillary arch collapses into crossbite (Figure 26-3).

 FIGURE 26-3
FIGURE 26-3Data on the amount of skeletal change are not clear. Some believe the maxilla and its alveolar process are moved anteriorly and superiorly.17 Certainly, if the teeth are moved, some alveolar change occurs. Whether this is translated to the skeletal maxilla is not as well known. In one study a significantly higher percentage of distal step molar relationships in 5-year-olds was noted among digit suckers compared with children with no sucking habit.9
Treatment
Reminder Therapy
The second approach, reminder therapy, is appropriate for those who desire to stop the habit but need some help. The purpose of any treatment should be thoroughly explained to the child. An adhesive bandage secured with waterproof tape on the offending finger can serve as a constant reminder not to place the finger in the mouth (Figure 26-4). The bandage remains in place until the habit is extinguished. There are some parents who are reluctant to use the bandage as a reminder. They are concerned that it may come off during sleep and the child may swallow or aspirate the bandage. Therefore some clinicians use a mitten or a tube sock to cover the fingers of the hand. This is especially useful during sleeping hours. Other commercial products such as shirts that cover the hand or plastic sleeves that cover the thumb are available. Another approach is to paint a commercially available bitter substance on the fingers that are sucked. However, sometimes this type of therapy is perceived as punishment and may not be as effective as a neutral reminder. In conclusion, reminder therapy works by changing the sucking sensation enjoyed by the child.

 FIGURE 26-4
FIGURE 26-4Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


