23
The face and superficial neck
Chapter contents
23.1 Introduction
The surface anatomies of the face and neck and their supporting structures that can be palpated have been described in Chapter 20. It is now time to move to the structures that lie under the skin but which cannot be identified by touch starting with the neck and moving up on to the face and scalp.
23.2 The neck
23.2.1 The cervical vertebral column
The cervical vertebral column comprises the seven cervical vertebrae and the intervening intervertebral discs. These have the same basic structure as the thoracic vertebrae described in Section 10.1.1. Examine the features of the cervical vertebra shown in Figure 23.1 and compare it with the thoracic vertebra shown in Figure 10.3. You will see that cervical vertebrae have a small body and a large vertebral foramen. They also have two distinguishing features, a bifid spinous process and a transverse foramen, piercing each transverse process; the vertebral vessels travel through these foramina.
The first and second vertebrae are modified. The first vertebra, the atlas, has no body. Instead, it has two lateral masses connected by anterior and posterior arches. The lateral masses have concave superior facets which articulate with the occipital condyles where nodding movements of the head take place at the atlanto-occipital joints. The second cervical vertebra, the axis, has a strong odontoid process (or dens because of its supposed resemblance to a tooth) projecting upwards from its body. This process is, in fact, the body of the first vertebra which has fused with the body of the axis instead of being incorporated into the atlas. The front of the dens articulates with the back of the anterior arch of the atlas; rotary (shaking) movements of the head occur at this joint. The seventh cervical vertebra has a very long spinous process which is easily palpable.
The primary curvature of the vertebral column is concave forwards and this persists in the thoracic and pelvic regions. In contrast, the cervical and lumbar parts of the vertebral column are convexly curved anteriorly. These anterior curvatures are secondary curvatures which appear in late fetal life. The cervical curvature becomes accentuated in early childhood as the child begins to support its own head and the lumbar curve develops as the child begins to sit up. There is only a small degree of movement between adjacent cervical vertebrae. However, the cumulative effect is considerable and gives the neck its characteristic flexibility. When the neck is fully flexed, the cervical vertebrae are in a straight line.
23.2.2 Cervical fascial layers
The layers of connective tissue that form compartments between tissues or enclose muscles, for example, are impermeable to fluids such as blood and pus. Pathological fluids spread through the spaces between the fascial layers rather than piercing the fascial planes and infected material is able to track considerable distances from its point of origin.
Knowledge of the fascial planes and spaces used to be of considerable clinical significance for correct diagnosis and treatment of infective and inflammatory conditions. The accumulation of large quantities of pus from dental infections is now an uncommon event in developed countries owing to the availability of early treatment and the widespread use of antibiotics. Nevertheless, a knowledge of the fascial planes in the neck and their connections with tissue spaces in the floor of the mouth (see Section 25.3.4) is still of value to dentists practising in areas where primary treatment and antibiotics are not widely available. Fasciae are remarkably difficult to distinguish on conventionally preserved human cadavers. The fascial planes are described in Box 23.1.
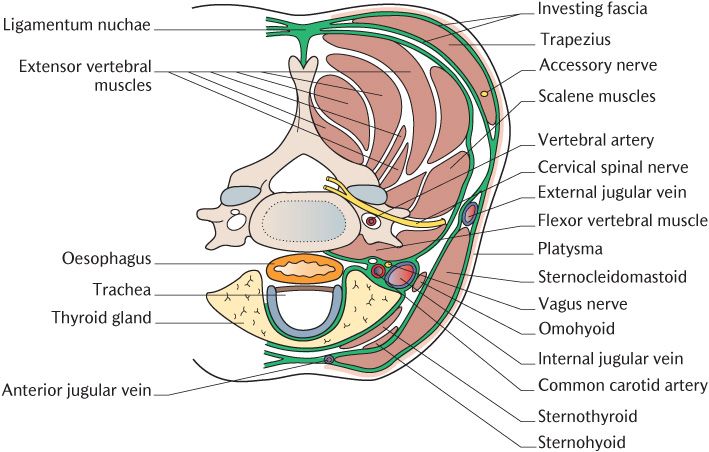
Fig. 23.1 The arrangement of the deep fascia of the neck shown on a horizontal section at the level of the sixth cervical vertebra.
Box 23.1 Fascial planes in the neck
Superficial fascia
The superficial fascia is the subcutaneous layer of loose connective tissue. It does not usually contain such large amounts of fat as the equivalent layer in the trunk but there may be as much in some individuals.
Deep fascia
As shown in Figure 23.1, the deep fascia comprises the layers of connective tissue surrounding the deeper structures of the neck. The investing layer of the deep cervical fascia is arranged like a cylinder around the neck, lying immediately deep to the superficial fascia. It attaches inferiorly to the scapula, clavicle, and the manubrium sterni. Posteriorly, its upper attachment is to the external occipital protuberance, superior nuchal line, and mastoid process of the skull; the fascia splits to enclose the attachments of the trapezius and sternocleidomastoid muscles. It also splits into two layers to form the parotid capsule, enclosing the parotid gland between the mastoid process and the posterior border of the mandibular ramus. Anteriorly, the investing layer is attached to the lower border of the mandible.
The prevertebral fascia is a tough membrane covering the anterior aspect of the flexor muscles of the cervical spine. It extends from the base of the skull downwards to the third thoracic vertebra. Laterally, it passes in front of the lateral vertebral (scalene) muscles and continues backwards, enveloping the extensor vertebral muscles. The carotid sheath of each side consists of a tube of connective tissue surrounding the common carotid artery and internal carotid artery above the bifurcation, the internal jugular vein, and vagus nerve. The sheath is attached to the base of the skull around the opening of the carotid canal and continues downwards along the common carotid artery to fuse with the connective tissue around the arch of the aorta.
23.2.3 Cervical muscle groups
There are six main groups of neck muscles, the superficial muscles, the suprahyoid and infrahyoid muscles, and the flexors, extensors, and lateral vertebral muscles of the cervical spine. Only the superficial and suprahyoid and infrahyoid muscles will be described as the other groups have no direct relevance to clinical dentistry. The arrangement of the flexor, extensor, and lateral vertebral muscles groups can be seen in Figure 23.1.
Superficial muscles
Platysma
The platysma is the first muscle you will encounter beneath the skin if you have the opportunity to dissect a human cadaver. Each muscle is a broad sheet arising from the fascia covering the pectoralis muscles on the front of the thorax. Their fibres sweep upwards and medially in the superficial fascia across the clavicle and into the side of the neck as shown in Figure 23.1. Figure 23.8 shows their superior attachments into the lower border of the mandible and into the skin and muscle of the lower lip, especially towards the angle of the mouth. The platysma muscles belong to the muscles of facial expression (see Section 23.3.2) and are innervated by the cervical branches of the facial nerve. The muscles vary in size and may be absent. Platysma tightens the skin of the neck. If present, the fibres inserting into the lip depress the corners of the mouth.
Sternocleidomastoid
We have already encountered the bulky strap-like sternocleidomastoid muscle when considering the surface anatomy in Chapter 20. As shown in Figure 20.8, it passes obliquely across the side of the neck, dividing the anterior and posterior triangles. Figure 23.8 illustrates its attachments to the manubrium sterni by a tendinous sternal head and to the upper surface of the medial third of the clavicle by a fleshy clavicular head; the two heads blend as they pass upwards. The muscle is attached superiorly to the lateral aspect of the mastoid process and the lateral part of the superior nuchal line. It receives its motor innervation from the spinal accessory nerve. When the muscle contracts, the mastoid process is brought towards the sternum. When the two muscles act together, they flex the neck but at the same time extend the head; the head is drawn forwards, but the face remains vertical. If only one muscle is active, the back of the head is drawn towards the shoulder of the same side, thus turning the face towards the opposite side and tilting it upwards.
Trapezius
Again this is a muscle already met in Chapter 20 (see Figure 20.8). Each muscle is a large flat triangular muscle; the muscles of the two sides form a trapezium from which the name of the muscle is derived. Each muscle is attached from the superior nuchal line and external occipital protuberance above and the ligamentum nuchae between the extensor muscles and the spinous processes of the seventh cervical and all the thoracic vertebrae. Figure 23.8 shows the superior fibres in the neck pass downwards and laterally to attach to the lateral third of the clavicle. The inferior fibres running laterally from the posterior thoracic wall converge and attach into the scapula. This muscle is also innervated by the spinal accessory nerve. The muscle mainly functions to control the position of the scapula working with other thoracic and upper limb muscles. When the scapula is fixed, the upper fibres in the neck extend the head and neck.
The accessory nerve
The origins and intracranial course of the spinal accessory nerves have already been described in Section 18.11. Each nerve exits through the jugular foramen and slopes downwards and backwards to the upper part of the sternocleidomastoid muscle. It runs through the muscle to emerge in the posterior triangle which it crosses to enter the trapezius muscle.
The suprahyoid muscles
This group is made up of four pairs of muscles, the mylohyoid, geniohyoid, stylohyoid, and digastric muscles. They all attach to the hyoid bone below and to the mandible, styloid, and mastoid processes above. The muscles are illustrated in Figure 23.2 which should be examined as you read the following description.
The mylohyoid muscle passes medially from the mylohyoid line of the mandible to attach to the hyoid bone posteriorly and to meet its opposite number at the median raphe; the anterior components of the muscles form the floor of the mouth. Each digastric muscle has two muscle bellies joined by a tendon. The anterior belly is attached to the digastric fossa on the inside of the mandible body close to the midline and runs backwards towards the hyoid bone. The posterior belly attaches to the mastoid notch and runs forward towards the hyoid bone. As you can see in Figure 23.2, the two bellies are joined by the intermediate tendon which runs through a fibrous sling attached to the hyoid bone. The entire muscle thus forms a shallow V. The stylohyoid muscles are largely covered by other muscles and the geniohyoid muscles run deep to the mylohyoid so are not superficial structures. These muscles are described as part of the floor of the mouth in Chapter 25.
The suprahyoid muscles elevate the hyoid bone and laryngeal skeleton during swallowing; they also play a role in opening the mouth when they act from a fixed hyoid bone to pull down on the mandible (see Chapter 26). Their nerve supply is complicated because different muscles arise from different pharyngeal arches (Table 21.1). The mylohyoid and anterior digastric are first arch muscles and are, therefore, innervated by the mandibular trigeminal nerve. The stylohyoid and posterior digastric are second arch derivatives and therefore obtain their motor innervation from the facial nerve. The embryology of the geniohyoid is uncertain; it is innervated by the first cervical nerve.
The infrahyoid muscles
The sternohyoid, sternothyroid, thyrohyoid, and omohyoid muscles make up this group of four pairs of strap-like muscles running from the hyoid to the sternum and clavicle via the laryngeal skeleton. The muscles can be traced in Figure 23.2. The two parts of the name of each muscle tell you their attachments, e.g. sternohyoid attaches to the sternum and hyoid. They depress the hyoid bone and laryngeal skeleton on completion of swallowing. They also fix the hyoid so that the suprahyoid muscles can act on the mandible using the hyoid as a fixed attachment. They are supplied by branches of the cervical spinal nerves through the cervical plexus (see Section 23.1.4). Further details of this muscle group are provided in Box 23.2 for those that require it.
The lateral vertebral muscles, the anterior, medius, and posterior scalene muscles shown in Figure 23.1, attach to the transverse processes of the cervical vertebrae and run downwards and outwards to the upper two ribs. They laterally flex the cervical vertebrae as their name implies, but can act as accessory muscles of inspiration (see Section 11.4.2).
Box 23.2 The infrahyoid muscles
The sternohyoid muscles are the most superficial and run from the manubrium sterni and adjacent end of the clavicle to the body of the hyoid bone. They cover the sternothyroid and thyrohyoid muscles. The sternothyroid runs from the manubrium sterni to the oblique line on the thyroid cartilage. The thyrohyoid muscle continues this layer upwards from the oblique line to the lower border of the greater cornu and body of the hyoid bone. Each omohyoid muscle consists of two bellies. The inferior belly arises from the scapula and passes forwards across the lower part of the neck deep to sternocleidomastoid. The superior belly attaches to the body of the hyoid lateral to sternohyoid and runs directly downwards where it attaches to the intermediate tendon linking it to the inferior belly. The intermediate tendon is held in place by a fibrous loop attached to the clavicle and first rib.
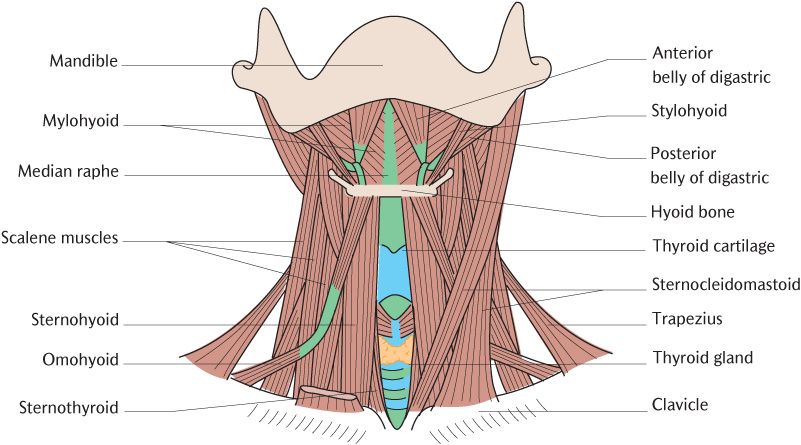
Fig. 23.2 The infrahyoid muscles and some of the suprahyoid muscles. The right sternocleidomastoid has been removed for clarity.
The posterior triangle of the neck
The borders of posterior triangles have already been described in Chapter 20 and illustrated in Figure 20.8. The accessory nerve crosses the triangle almost vertically from the posterior border of sternocleidomastoid to the anterior border of trapezius. The four superficial branches of the cervical plexus (see below) emerge from the posterior triangle around the posterior edge of sternocleidomastoid.
23.2.4 Cervical spinal nerves
There are eight pairs of cervical spinal nerves. The first to seventh cervical nerves leaves the vertebral canal by passing above the vertebra of the same number; the first nerve emerges between the occipital bone and the atlas. The eighth nerve emerges between the seventh cervical and the first thoracic vertebrae. Each nerve, like all spinal nerves, then divides into a dorsal and ventral ramus.
The dorsal rami run posteriorly to supply the extensor muscles of the neck and the skin over the back of the neck and scalp. The dorsal ramus of each second cervical nerve forms a large cutaneous branch, the greater occipital nerve, which supplies the posterior aspect of the scalp as far as the vertex. The dorsal rami of the remaining cervical nerves have small cutaneous branches to the back of the neck.
The ventral rami of the first four cervical spinal nerves (C1–4) join to form the cervical plexus. The ventral rami of the remaining four cervical nerves and the first thoracic nerve (C5–T1) join to form the brachial plexus, the nerve supply to the skin and muscles of the upper limb.
The cervical plexus
The four ventral rami branch and rejoin as illustrated in Figure 23.3 to produce the cervical plexus. Deep branches from the plexus supply motor axons to the infrahyoid muscle group and some other muscles. The most important motor branch is the phrenic nerve to the diaphragm formed from the third, fourth, and fifth cervical nerves. Superficial branches are distributed to the skin of the front and sides of the neck and part of the side of the head. Further details of the cervical plexus are provided in Box 23.3 if your curriculum demands them.
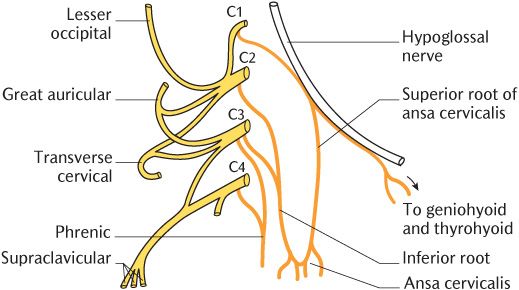
Fig. 23.3 The cervical plexus. Sensory branches are shown in yellow and motor branches in orange.
23.2.5 Arteries in the neck
The common carotid arteries and vertebral arteries pass through the neck on each side to supply the head, including the brain as already described in Section 15.5. The carotid arteries arise from the aortic arch in the thorax and the vertebral arteries are branches of the subclavian arteries. The common carotid arteries divide high in the neck into the external and internal carotid arteries. Branches from the vertebral and external carotid arteries supply the neck itself.
The deep branches are:
• A communicating branch from the first cervical nerve to the hypoglossal nerve carrying motor axons to the geniohyoid and infrahyoid muscles. The nerves supplying the geniohyoid and thyrohyoid run to their destination in the hypoglossal nerve. Axons to the remaining infrahyoid muscles leave the hypoglossal nerve in the superior root of the ansa cervicalis branch (also called the descendens hypoglossi) which passes along the front of the carotid sheath to join the inferior root to form the ansa cervicalis.
• Muscular branches pass from all four cervical nerves to the prevertebral muscles.
• Proprioceptive branches pass to the sternocleidomastoid and trapezius muscles, respectively.
• The inferior root of the ansa cervicalis (or descendens cervicalis) from the second and third cervical nerves joins the superior root nerve to form the ansa cervicalis. Branches of the latter supply the infrahyoid muscles, except thyrohyoid.
• The phrenic nerve, derived mainly from the fourth cervical nerve with small additions from the third and fifth nerves, runs vertically downwards over the anterior scalene muscle and then passes behind the subclavian vein to enter the mediastinum. Its further course is described in the Section 10.2.4.
The superficial branches of the cervical plexus hook around the posterior border of sternocleidomastoid and radiate outwards to supply skin over the neck, a small area of scalp, and an area of the face. Their distribution is shown in Figure 23.12.
• The lesser occipital nerve derived from the second cervical nerve runs upwards along the posterior border of sternocleidomastoid to supply to skin of the scalp behind the auricle.
• The great auricular nerve from the second and third cervical nerves runs upwards to supply the skin of the auricle and of the face over the parotid gland and angle of the mandible.
• The transverse cervical nerve, another derivative from the second and third nerves, runs forwards to supply the skin of the side and front of the neck.
• The supraclavicular nerves, derived from the third and fourth cervical nerves, pass downwards and fan out to supply skin over the chest and shoulder.
The common carotid artery
The origin of the right and left common carotid arteries is different on each side. On the right side, the brachiocephalic trunk divides after a short course into the right common carotid and subclavian artery whereas the left common carotid and subclavian arteries are direct branches of the aortic arch (see Chapter 12, Figure 12.10).
Each common carotid artery leaves the thorax and ascends through the neck alongside the corresponding internal jugular vein and vagus nerve. These three structures are bound together by the carotid sheath. As illustrated in Figure 23.4, the common carotid arteries bifurcate into the internal and external carotid arteries; the level of bifurcation is usually about the level of the upper border of the thyroid cartilage or hyoid bone. The internal carotid artery continues upwards within the carotid sheath whereas the external carotid artery leaves the sheath and thus becomes external to it.
The carotid sinus is a dilatation on the common carotid artery at its bifurcation which continues a little way up the internal carotid branch. The carotid sinus contains baroceptors monitoring blood pressure innervated by the carotid branch of the glossopharyngeal nerve. The carotid body is usually situated behind the sinus or between the internal and external carotid arteries and is only a few millimetres in width. It contains chemoreceptors responding to oxygen and carbon dioxide levels in the blood and is also innervated by the glossopharyngeal nerve. Its carotid branch forms the afferent arc of cardiovascular and respiratory reflexes in response to altered blood chemistry or pressure.
The internal carotid artery
The internal carotid arteries are shown in Figure 23.5. They ascend on either side of the pharynx without branching to enter the base of the skull through the carotid canals. Each artery follows an S-shaped course through the canal, tracking superiorly at first, then turning medially before resuming its superior course to enter the middle cranial fossa just above the foramen lacerum. The internal carotid arteries terminate by branching into the anterior and middle cerebral arteries which are described in Chapter 15 and illustrated in Figure15.24.
The external carotid artery
Each external carotid artery ascends through the upper part of the neck supplying numerous branches to adjacent structures. They are illustrated in Figure 23.4; follow their course as you read the description. Each external carotid artery enters the parotid gland at about the level of the angle of the mandible and terminates within the substance of the parotid glands by dividing into two terminal arteries. Each external carotid artery has eight branches; some of these are of little direct importance to clinical dental practice.
The superior thyroid arteries branch off almost immediately after the bifurcation, then descend and spread out to supply the anterosuperior aspects of the thyroid gland. They also supply small penetrating branches that supply the larynx.
The ascending pharyngeal arteries arise at about the same level as the superior thyroid arteries but are hidden on the medial aspect of each external carotid artery; they are, therefore, not visible in Figure 23.4. These arteries ascend on either side of the pharynx and supply it as they do so. They terminate by contributing to the blood supply of the palatine tonsils.
The lingual and facial arteries may arise separately or from a short common stem. As their names imply, they supply the tongue and face, respectively. The lingual arteries pass deep to the mandible and cross the floor of the mouth to ascend into the tongue. They supply the tongue and the floor of the mouth and their course here is described in Section 25.3.4. The course of the facial artery is described in Section 23.2.1. The lingual and facial arteries also supply the bone of the mandible through periosteal branches along their course.
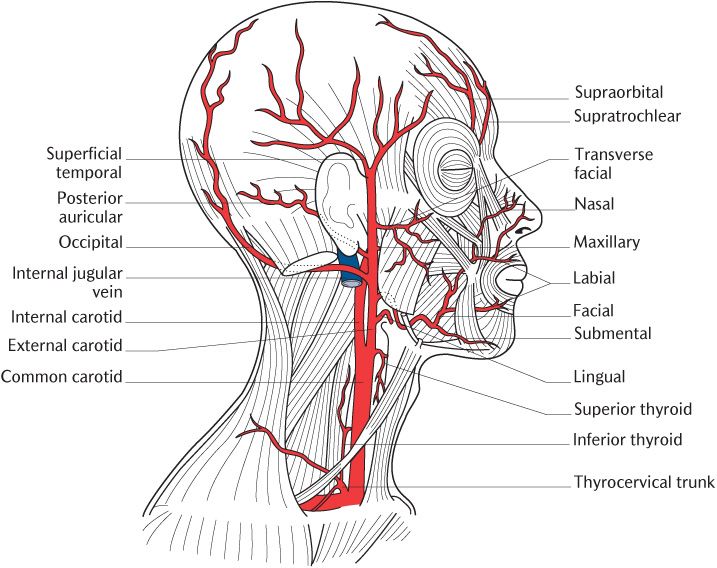
Fig. 23.4 The carotid arteries and their branches.
The occipital arteries supply skin over the back of the neck and scalp. The posterior auricular arteries supply the scalp behind the ears and have a stylomastoid branch that enters the stylomastoid foramen to supply the tympanic cavity.
The two terminal br/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


