22
The skull
Chapter contents
22.1 Introduction
Dental students and practitioners require a sound knowledge of the structure, growth, and development of the skull as a whole. The structure of the skull can be examined and studied more efficiently if you have access to a dried skull or one of the very good plastic replica skulls which are now available; you can identify the structures on the diagrams accompanying the following descriptions and examine a skull at the same time to appreciate the size and relationships of individual components.
This chapter outlines the basic principles of the development and structure of the skull and includes some reference to individual bones where this makes understanding easier. The more detailed aspects of particular regions of the skull will be covered in the appropriate chapter describing the whole anatomy of that region; it is much easier to learn the parts of the skull in context of overall structure and function rather than learning a long list of bones, foramina, and muscle attachments in isolation from the related soft tissue structures. Only the maxilla and mandible which are bones of significant clinical importance are described as separate bones.
22.2 Components and subdivisions of the skull
As already demonstrated in Chapter 20, the skull is the structural basis for the anatomy of the head. The skull has many functions.
• It encloses and protects the brain.
• It provides protective capsules for the eyes and middle and inner ear.
• It forms the skeleton of the entrances to the respiratory and gastrointestinal tracts (GIT) through the nose and mouth, respectively.
Those skull components that form the entrance to the GIT also house and support the teeth and soft tissues of the oral region as part of this function.
As already outlined in Chapter 20, the skull is made up of several bones joined together to form the cranium which articulates with the separate mandible forming the lower jaw at the temporomandibular joints. The cranium specifically refers to the skull without the mandible; the terms ‘skull’ and ‘cranium’ are not strictly synonymous but they are frequently used as though they are.
The cranium can be subdivided into the braincase enclosing the brain and the facial skeleton. The roof and sides of the braincase, the cranial vault, are formed by relatively thin, smooth, curved bones. The more complex bones of the upper facial skeleton form the walls of the orbits, the nasal cavity, and the upper jaws. The mandible forms the lower jaw to complete the bony components around the oral cavity. A strong bar of bone, the zygomatic arch, runs on each side from the lower lateral part of the cranial vault to the side of the upper facial skeleton. The braincase, upper facial skeleton, and mandible can be identified very easily on a dried skull.
The cranial base or chondrocranium which forms the floor of the braincase and the roof of the nasal cavity, and houses the inner ear is much less easy to differentiate instinctively. Only the posterior part of the cranial base can be seen in an intact skull when viewed from the underside because the anterior part of the cranial base is obscured by the upper facial skeleton which is attached to its underside. Dried and model skulls usually have a detachable skull cap which can be removed for examination of the inside of the braincase. The bones forming the whole length of the cranial base can be seen in the floor of the braincase when the skull cap is removed. Recall from Chapter 15 (Figure 15.1) that the floor of the cranial cavity is arranged as three step-like hollows—the anterior, middle, and posterior cranial fossae.
22.2.1 Evolution and development of the skull
The division of the cranium into cranial vault, facial skeleton, and cranial base is based upon their developmental and evolutionary history in addition to the structural reasons. The bones that contribute to the skull can be divided on developmental grounds into the chondrocranium, where bones develop first as a cartilage template which is then replaced by bone and dermal bones which ossify directly in mesenchyme without an intervening cartilaginous stage.
In early vertebrates, the chondrocranium was a well-developed structure, forming protective boxes around the brain and organs of special sense as well as contributing to the upper and lower jaws through the pterygoquadrate and Meckel’s cartilages and their replacing bones (see Section 21.5.1). The chondrocranium is greatly reduced in most modern vertebrates but still forms major skull components. In mammalian skulls, the chondrocranium and its replacement bones are restricted to the cranial base and the capsules around the inner ears and nasal cavities. The chondrocranial elements that form the upper and lower jaw in non-mammalian vertebrates take no real part in their formation and structure in modern mammals; the malleus and incus of the middle ear are their only derivatives. The bones that develop from cartilaginous precursors of the chondrocranium mineralize by a process of endochondral ossification. This term is not strictly accurate as the cartilage actually grows, then bone replaces the older parts of the growing cartilage to consolidate the structure. The most accurate term for bones that mineralize in cartilage is cartilage-replacing bones. Note that cartilage-replacing bones form the whole of the post-cranial skeleton, except the clavicles.
Dermal bones, as their name implies, were originally bony plates formed as protective armour plating within the dermis, the connective tissue component of skin; during evolution, they were added to the skull to provide further protection for the brain and sense organs and to complete the jaws. The cranial vault, the lower jaw, and the upper facial skeleton, apart from some of the bones around the nose, are made up of dermal bones. Dermal bones mineralize by a process called intramembranous ossification. They are also referred to as membrane bones or intramembranous bones, but dermal bone is the most accurate and reflects the evolutionary origin of these bones. The clavicles are the only other dermal bone found in the human skeleton.
The growth of the different compartments of the skull is determined to a large extent by the growth of the tissues they enclose (see also Section 33.2). The growth of the cranial vault is largely determined by growth of the brain and is also referred to as the neurocranium whereas growth of the facial skeleton is related to the growth rate of viscera and thus becomes the viscerocranium. The cranial basal grows at an intermediate rate to accommodate the different growth rates of neural tissue above and viscera below. The terms ‘neurocranium’ and ‘viscerocranium’ tend to be used more when describing the growth and development of the skull. The neurocranium grows faster than the facial skeleton because the CNS grows at a much more rapid rate than the rest of the body initially. The different growth rates account for the change in proportion of the skull throughout growth. A baby’s face seems very small whereas its braincase and eyes are extremely large; the proportions change as growth proceeds until the adult proportions are achieved when the forehead occupies the upper third of the skull, the upper facial skeleton the middle third, and the mandible the lower third.
22.2.2 Joints in the skull
The joints between the dermal bones of the upper facial skeleton and of the cranial vault are fibrous sutures whereas the joints in the central regions of the cranial base consist of hyaline cartilage and are termed synchondroses. The sutures and synchondroses are named from the contributory bones in many cases, e.g. the zygomaticomaxillary suture; the spheno-occipital synchondrosis. In some instances, they are named from their shape (the lambdoid suture resembles the Greek letter lambda λ) or position (the coronal suture passes across the crown).
Sutures and synchondroses in the developing skull function as growth sites but do not allow movement (see Sections 33.3.1 and 33.4.1). However, at the time of birth, the sutures of the cranial vault are sufficiently flexible to allow some overriding of adjacent bones which enables the head, usually the first part to be born, to pass more readily through the vagina. Synchondroses are replaced by bone as growth ceases and all traces are obliterated. Sutures persist and characteristically the edges of adjacent bones are wavy in outline due to small finger-like projections from adjacent bones which interdigitate to produce a strong interlock between them. Sutures are overgrown by bone later in life, usually from the inner surface to the external surface, and may be difficult to distinguish on the skull of an elderly person; suture obliteration can give useful information about age in forensic dental examinations.
22.3 Let’s build a skull
From the outline of the skull and study of surface anatomy presented in Chapter 20, you will appreciate that some bones contributing to the skull are relatively simple in shape whereas others are complex and made up of multiple parts. These complex bones often contribute to more than one of the three basic compartments of the skull. A really excellent way to understand the skull, its component bones, and the contribution of complex bones to different parts of the skull is to build a skull from scratch. We can do this by studying the figures that follow. Figures 22.2 to 22.6 illustrate the complete skull from the anterior, lateral, inferior, internal, and superior views. Figure 22.7 will illustrate the sequential build-up of the skull as bones are added. As each bone is added to the skull, identify the new addition in Figure 22.7 to gain an overall view of where it is, then study the different views of the skull in Figures 22.2 to 22.6 to identify the components of the bone in question and its contribution to different views of the skull.
As described in Section 33.2, the cranial base and the capsules housing the organs of special sense are the first parts of the skull to form. The dermal bones forming the braincase and facial skeleton are then added to the cranial base. We will build our skull following the actual developmental sequence, starting with the cranial base, then adding the facial skeleton and cranial vault.
22.3.1 The cranial base
The sphenoid bone
The sphenoid bone is the key bone of the cranial base and all other skull components are attached to it either directly or indirectly. It is one of the first bones to form in the developing skull. The sphenoid also contributes to the walls of the orbit and nasal cavities in the facial skeleton and to the cranial vault. Study the three views shown in Figure 21.1 and on a skull, if possible, and identify:
• The body;
• Two greater wings;
• Two lesser wings;
• Two pterygoid processes.
The centrally placed body is approximately cuboidal; it is actually hollow and contains the two sphenoidal air sinuses. As you can see in Figure 22.1A, the superior surface of the body has a concavity, the pituitary fossa, which houses the pituitary gland. Note particularly in Figures 22.1B and 22.1C, the laterally projecting lesser and greater wings of the sphenoid; each lesser wing is above the greater wing and is separated from it by the superior orbital fissure. This fissure transmits the oculomotor, trochlear, abducens, and ophthalmic division of the trigeminal nerves from the cranial cavity into the orbit on each side. Not surprisingly, the greater wing projects further laterally than the lesser wing above it. Each greater wing is curved upwards and laterally. Its inner face forms the anterior wall and part of the side wall of the middle cranial fossa (Figures 22.4 and 22.5) and its outer face contributes to the orbit (Figure 22.2) and forms part of the lower lateral wall of the cranial vault (Figure 22.3). In Figure 22.1A, identify the foramen rotundum and ovale on each side in the root of the greater wing where it joins the body. They transmit the maxillary and mandibular divisions of the trigeminal nerve, respectively. The lesser wings of the sphenoid form part of the anterior boundary of the middle cranial fossa. Note in Figure 22.1B, the two optic canals in the bases of the lesser wings; the optic nerves pass through these canals to the orbits. Figures 22.1B and 22.1C show the pterygoid processes hanging down from the sphenoid body and roots of the greater wings. Each process consists of a medial and lateral pterygoid plate. These can be seen on lateral (Figure 22.3) and inferior views (Figure 22.4) of the skull. The sphenoid bone is the first bone to appear on the schematic construction of the skull shown in Figure 22.7 and is the only one present in Figure 22.7A.
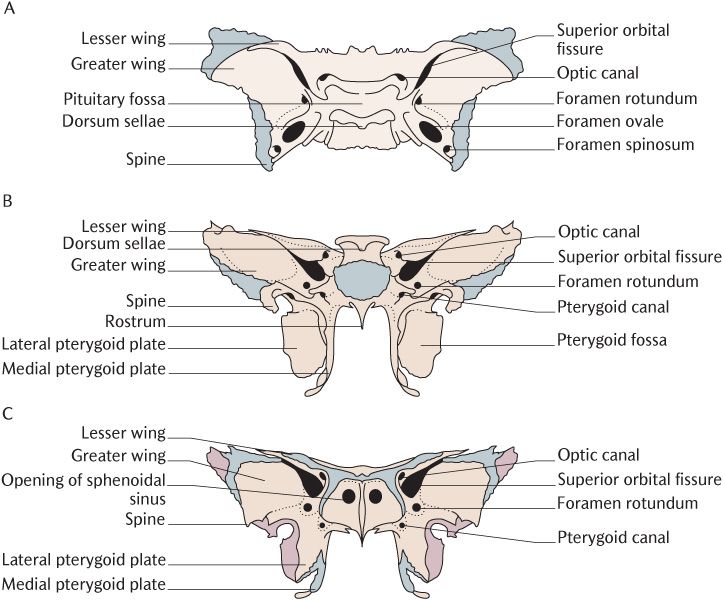
Fig. 22.1 The sphenoid bone. A) Superior view; B) Posterior view; C) Anterior view. Dark grey indicates areas of articulation with other bones.
The occipital bone
The cranial base is extended backwards from the body of the sphenoid by the basal part of the occipital bone as shown in Figure 22.7B. This bone is somewhat simpler than the sphenoid bone. Its two major components are the basal part (or basiocciput), a cartilage-replacing bone, and the squamous part which is a dermal bone; the two fuse during development.
The basiocciput bone is easily recognized because it is pierced by the huge midline foramen magnum which you can see very clearly in Figures 22.4 and 22.5. This foramen marks the continuation of the medulla and spinal cord. You are unlikely to find a joint between the body of the sphenoid and the basiocciput on most skulls. The spheno-occipital synchondrosis is a crucial growth site in the chondrocranium during development (see Section 33.2.3). This joint is totally overgrown when growth at this site ceases around the time of puberty and is, therefore, not visible after this age. The colouration of different bones in Figures 22.4 and 22.5 does indicate its location. In Figure 22.4, you can see two prominent hemispherical bulges on the underside of the basiocciput either side of the foramen magnum. These occipital condyles are the superior articulatory surfaces of the atlanto-occipital joints and articulate with concave surfaces on the superior aspect of the atlas, the first cervical vertebra; flexion and extension (nodding movements) of the head on the neck take place here.
The posterior rim of the foramen magnum is formed by the basiocciput which blends posteriorly with the squamous occipital bone; no joint is visible. The squamous occipital bone forms the posterior part of the floor of the posterior cranial fossa (Figures 22.4 and 22.5) and then curves backwards and upwards to form the posterior aspect of the cranial vault (Figure 22.3). It is roughly triangular in outline and its upper borders and apex meet the parietal bones at the lambdoid suture shown in Figures 22.3 and 22.6.
The temporal bone
The temporal bone is the next bone to be added to our growing skull as shown in Figure 22.7C. The temporal bone is another bone where some parts form as cartilage-replacing bone and others as dermal bones and later fuse. Figure 22.8 shows lateral, inferior, and medial views of the temporal bone. Its different parts are the petrous, mastoid, squamous, tympanic, and styloid; identify them in the figure and a skull.
The thick wedge-shaped petrous temporal bone that houses the middle and inner ear is the major contribution to the cranial base. It is most obvious in Figure 22.8B. Once you have identified its shape from Figure 22.8, you should be able to locate it in Figures 22.4 and 22.5 too. Note in Figures 22.7C and 22.5 how the wedge fits in between the posterior part of the greater wing of the sphenoid and anterior margin of the basiocciput on each side. The gap with a jagged (lacerated) outline where the three bones meet is the foramen lacerum. The upper opening of the bony carotid canal opens high in its posterior wall above the level of the cartilage in life. The carotid canal is a wide S-shaped channel passing through the petrous bone which transmits the internal carotid artery. The foramen lacerum does not exist in life as it is plugged with cartilage remnants from the development of these cartilage-replacing bones.
As you can see in Figure 22.8C, there is an obvious foramen on the medial aspect of the petrous temporal bone; this is the internal auditory meatus through which the vestibulocochlear nerves travel to the inner ear accompanied by the facial nerves. The facial nerves continue on through the middle ear where they make an abrupt 90° bend to exit through the stylomastoid foramen on the inferior surface of the petrous bone seen in Figure 22.8B. The upper and medial surfaces of the petrous bone meet almost at right angles. This edge is the boundary between the middle and posterior cranial fossae seen in Figure 22.5; the superior surface forms the posterior floor of the middle fossa and the medial surface the anterior wall of the posterior cranial fossa.
The tympanic plate is a small flat area that forms the anterior wall of the external auditory meatus, the wide canal entering the petrous temporal bone from its lateral aspect as shown in Figures 22.8A and 22.3.
The styloid process is a thin pointed bony spike about 2 to 3 cm long and is visible on all views in Figure 22.8. It is often broken off dried skulls, especially those that have been handled by generations of dental students, but its root is usually still identifiable. This process develops from the second pharyngeal arch cartilage (see Section 21.5.1) and several muscles and ligaments are attached to it; these will be described in later chapters.
As Figure 22.8A shows, the mastoid part is the posterior area of the temporal bone and the mastoid process projects inferiorly from it. As already described in Chapter 20 (Figure 20.8), the mastoid process is the superior attachment of the sternocleidomastoid muscle. Figure 22.8B also shows the mastoid notch, a deep groove on the medial side of the process for the attachment of the posterior belly of the digastric muscle.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


