Occlusal Development, Malocclusions, and Preventive and Interceptive Orthodontics
Bengt Mohlin, Anna Westerlund, Maria Ransjö, and Jüri Kurol
Craniofacial development and growth
Dental occlusion is strongly influenced by the craniofacial development and growth which determine size and relative proportions of the jaws. The craniofacial region is one of the most complex parts of the body. The development and growth of structures in the craniofacial complex is under genetic control and influenced by epigenetic and environmental factors. Not surprisingly, dentofacial deformities, large disproportions between the jaws, and severe discrepancies in occlusion are caused by disturbances in the development and growth [1,2].
Development of the head and face starts early during embryogenesis with interactions between the three germ layers. Formation, migration, and differentiation of the cranial neural crest cells, a multipotent cell population, are critical events in development of the craniofacial region. Expression of specific genes and interactions between signaling pathways regulate the continued development of the neural crest cells. They give rise to most of the bones, connective tissues, and cartilage in the craniofacial region and are also involved in tooth development. Mutations of regulatory genes cause craniofacial anomalies, sometimes associated with disturbed tooth development (see Chapter 4). Nearly a third of all birth defects involve the craniofacial complex [1].
The human face is largely already recognizable after the seventh prenatal week, even if the facial structures are not proportional or completely developed. The fetus has a proportionally large head; at 2 months it is approximately 50% of the body length but the proportions change over time due to differences in growth rate. The relative size of the head compared to the body length is approximately 25% at birth, decreasing to approximately 12% in an adult (Figure 21.1). Also the neurocranium to the face proportions change during the prenatal and postnatal period due to differential growth. The fetus has a large cranium compared to the face and this is also noticeable in the newborn (Figure 21.2). Since growth rates are differential, the neurocranium has nearly completed its growth in 5‐year‐old children while the jaws have reached approximately 50% of adult size [2].
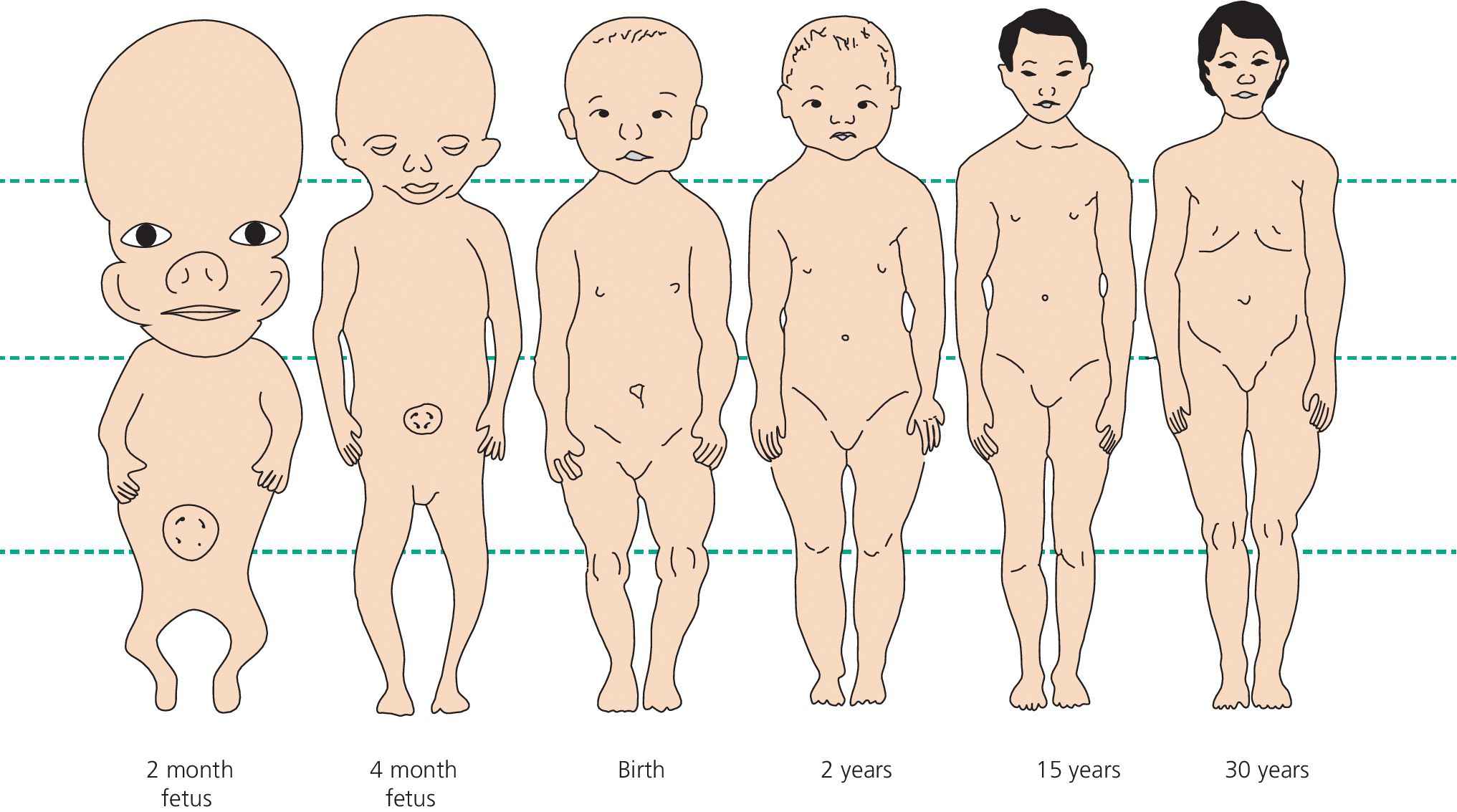
Figure 21.1 Changes in body proportions during development and growth.
(Redrawn from WJ Robbins et al. Growth. Yale University Press 1928, figure 63. Reproduced with permission of Yale University Press.)
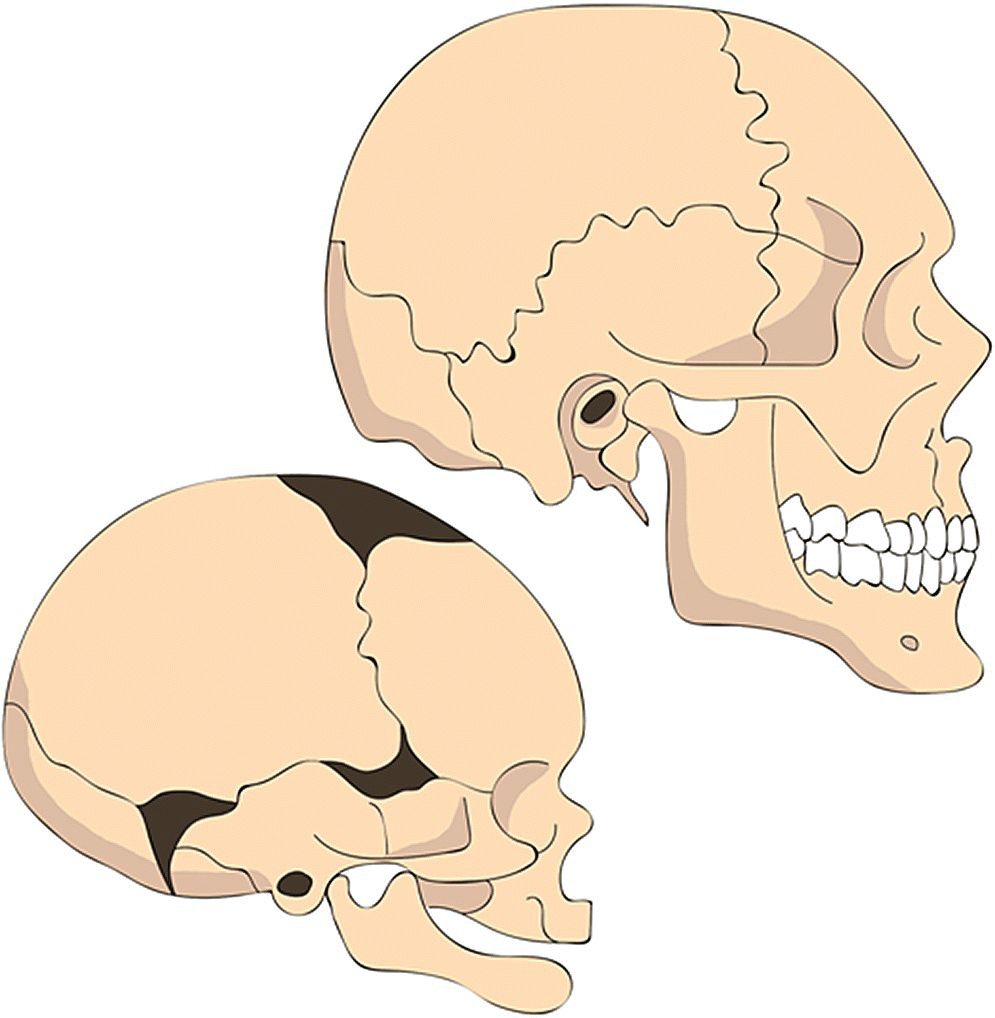
Figure 21.2 Changes in proportions of the head.
(Redrawn from GH Lowery, Growth and development of children, 6th ed. Chicago: Mosby, 1973. Reproduced with permission of Elsevier.)
The bones in the cranial base are formed by endochondral ossification, starting with initial cartilage models. Cartilage remnants (synchondroses) between the ossification centers are important growth sites in the cranial base. The cranial vault and facial bones (including maxilla and mandible) are formed by direct intramembranous ossification with fibrous sutures being the important sites for bone apposition and remodeling. The sutures and synchondroses between the different craniofacial bones fuse and terminate growth at different times. Premature closure of synchondroses or sutures may cause detrimental defects in growth and development depending on closure time and position [1].
By application of tensile forces it is possible to increase apposition of bone in a suture (before closure). Orthodontists can take advantage of this mechanism, e.g., when treating skeletal cross bites with a rapid maxillary expansion of the midpalatal suture.
General principles discussed in the growth and development of the craniofacial skeleton are displacement, due to growth and remodeling in sutures, and apposition and resorption processes at bone surfaces. Since the maxilla is attached to the anterior cranial base, whereas the mandible is suspended under the middle cranial fossa, growth of the cranial base is of major importance for the intermaxillary relations and, thus, for development of the occlusion. The maxilla is displaced downward and forward in relation to the anterior cranial base by growth and adaptation in the maxillary sutures. The sagittal relation between the jaws is maintained by marked growth of the mandible (Figure 21.2).
Within the framework of this complex facial development, the erupting teeth come into interdigitation. However, individual variability in growth of the cranial base and the jaws is wide and the coordination of development in the various components is not always perfect. This is partly compensated for by dentoalveolar mechanisms.
Occlusal development
Primary dentition
At birth the crowns of the primary teeth have to a great extent been formed, while root development has not yet started (see Chapter 4). Thus, the gum pads are low and the palatal vault is flat. When the jaws are closed there is normally contact only in the posterior region of the gum pads, and the mandible is retruded in relation to the maxilla. During the first year of life, however, the sagittal jaw relationship improves, allowing the incisors to erupt in a normal sagittal relation.
Occlusion in the posterior segments is first established around 16 months of age, when the primary first molars come into occlusal contact. Once a good intercuspidation in all three planes is achieved, the jaws are normally closed to the same position each time and normal development occurs. The established occlusion has a guiding role in the interrelation between the jaws and subsequently for the proper positioning of later erupting permanent teeth (canines and second molars). Further stabilization of the occlusion is achieved by the occlusion of the large mesiopalatal cusps of the maxillary second molars.
With the eruption of primary teeth the alveolar processes develop, and there is a considerable increase in facial height. The growth of the maxillary alveolar process also results in an increase in palatal height. The primary teeth erupt almost perpendicular to the jaw bases. The interincisal angle is approaching 180°, and the occlusal plane is flat. During development, the dentoalveolar segments generally move anteriorly in relation to basal structures of the jaws (Figures 21.2 and 21.3).
Figure 21.3 Facial growth in a normal girl from 2 months to 5 years 2 months of age. Superimposition was made on the nasion–sella line registered at sella. Note the magnitude of mandibular growth from a marked retruded position.
The primary dentition is characterized by half‐circular dental arches. The most conspicuous feature is the space surplus in the front region of both jaws, needed later to accommodate the broader permanent front teeth. Especially marked diastemata are often found between the lateral incisors and the canines in the maxilla and the canines and first molars in the mandible. These diastemata are referred to as “primate spaces.” The primary second molars erupt without proximal contact with the primary first molars. However, in most children these molars drift into proximal contact between the third and fourth years of life.
As to the basal relationships of the jaws, young children differ from older children and adults by being more maxillary prognate and mandibular retrognate. At 2 years, the overjet is on average 4 mm, with a range of 2–6 mm. With attrition of the teeth and growth of the mandible, the overjet shows a steady decrease up to the age of 5 years, where an edge‐to‐edge incisor relationship is common.
The primary incisors generally erupt into a rather deep overbite if there is no obstacle to hinder them. The individual variation is, however, wide. On average, the overbite decreases up to the age of 5–6 years as an effect of attrition.
The molar relations in the primary dentition may be divided into two types:
- the primary dental arches end in a mesial step, i.e., the distal surface of the second molar in the mandible is mesial to the corresponding surface in the maxilla (Figure 21.4, left)
- the dental arches end in the same vertical plan (Figure 21.4, right).
Figure 21.4 With a mesial step in the terminal plane of the primary dentition, the permanent molars may erupt directly into normal occlusion (left). If the primary dental arches end in the same vertical plane, the permanent molars will erupt into a cusp‐to‐cusp relation (right).
Both situations are favorable for the later guidance of the permanent first molar into normal occlusion. It should, however, be noted that the occlusion undergoes dynamic changes with jaw growth, with dental attrition, mesial drift of the dental arches on the jaw bases, and increased sagittal mandibular growth (Figure 21.3). At the time of eruption of the permanent first molar, a mesial step between the dental arches (Figure 21.4 left) is the most favorable.
Permanent dentition
The mixed dentition lasts from the eruption of permanent mandibular first incisors and first molars (about 6.5 years of age) until shedding of the last primary tooth (about 12 years of age) (see Chapter 5). The first permanent molars erupt in contact with the primary second molars. Thus, the establishment of molar sagittal relation will depend of the type of “step” between the distal surfaces of the maxillary and mandibular primary molars (Figure 21.4). The permanent first molars frequently establish a cusp‐to‐cusp relation. This relation normally turns into an Angle Class I after shedding of the primary second molars because of the greater leeway space in the mandible. In lateral segments the combined widths of the primary molars and canines are larger than the erupting successors and this extra space is called leeway space.
Sufficient space for the permanent molars is created by the sagittal growth of the jaws. Most important is the growth in the distal direction by apposition of bone on tuber in the maxilla and by the resorption at the anterior border of the mandibular ramus. Dental development and tooth eruption are not always coordinated in time with the growth of the jaws. Thus, the molars may erupt into an ectopic position.
Front teeth
The discrepancies in size between the primary and the permanent front teeth, amounting to 7 mm in the maxilla and 5 mm in the mandible, are neutralized in three ways:
- by utilizing space surplus (diastemata) normally present in the primary dentition
- by the proclined eruption path of the permanent incisors (Figure 21.5), which may add about 5 mm to the arch perimeter
- by a transversal increase in intercanine distance, which may add about 3 mm to the arch.
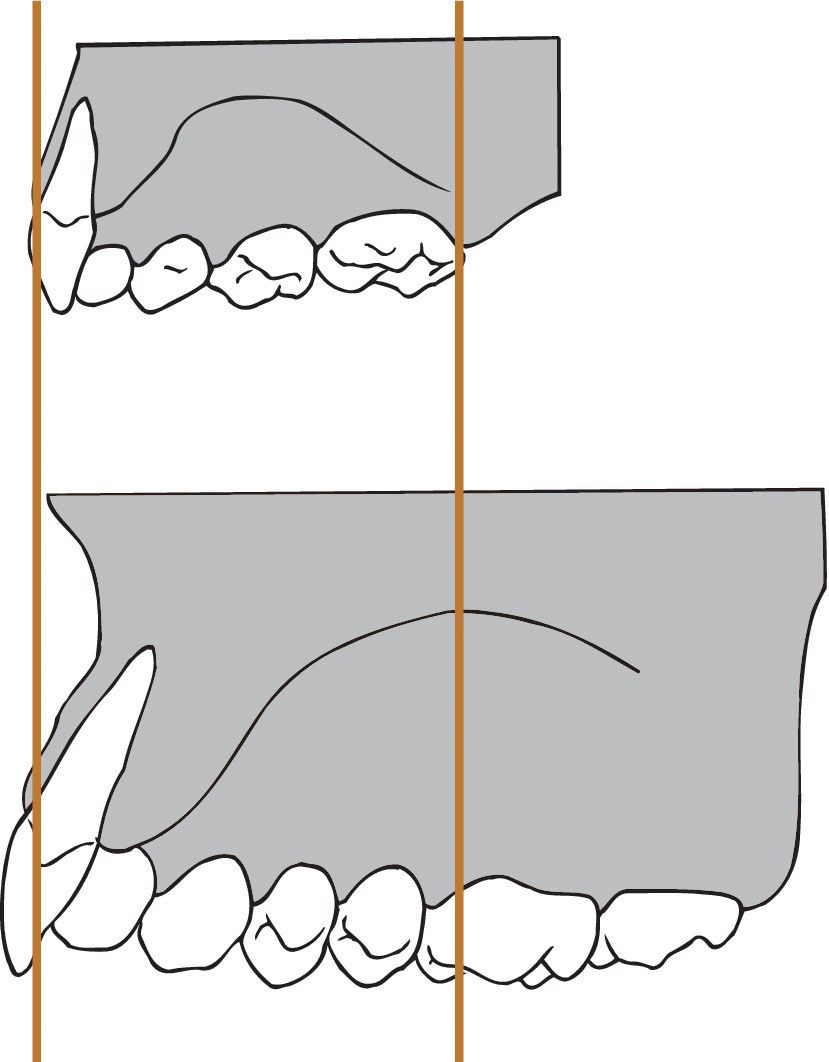
Figure 21.5 The permanent maxillary incisors erupt at a more labial inclination than their primary predecessors. Consequently, the dental arch becomes wider and longer.
Thus, the space for the permanent maxillary incisors is normally sufficient. However, in cases of insufficient diastemata between primary incisors, crowding may develop. In cases with anterior forced bite the proclination of the maxillary incisors is likely to be reduced. This may also contribute to development of crowding of the teeth. The mandibular incisors need less space (5 mm), but the diastemata are also smaller and the eruption path is steeper. Thus, a temporary crowding may exist until it is corrected by the increase in transversal width. However, lack of space at eruption of mandibular front teeth often occurs, and the amount of the spacing in the primary dentition is a good indicator for the prognosis of the later accommodation of the front teeth. Crowding is generally more pronounced in girls than in boys [3].
Lateral segment
When the primary molars and canines are shed, there is a net gain of space in the dental arches (leeway spaces 2.5 mm in the mandible, 1.5 mm in the maxilla) available for the eruption of the premolars and canines and also allowing a mesial migration of especially the mandibular molars to turn any cusp‐to‐cusp relations between first molars into a neutral relation. In the maxilla, the leeway space is needed to accommodate the canines, which are 2 mm larger than their predecessors (Figure 21.6). The increase in maxillary intercanine width in connection with eruption of the canines may also add some space. In the mandible, there is no corresponding gain in intercanine width related to canine eruption. The premolars will normally have sufficient space for eruption unless space is lost due to lack of space in the front, or because of early loss of primary molars due to caries or ectopic eruption of permanent first molars.
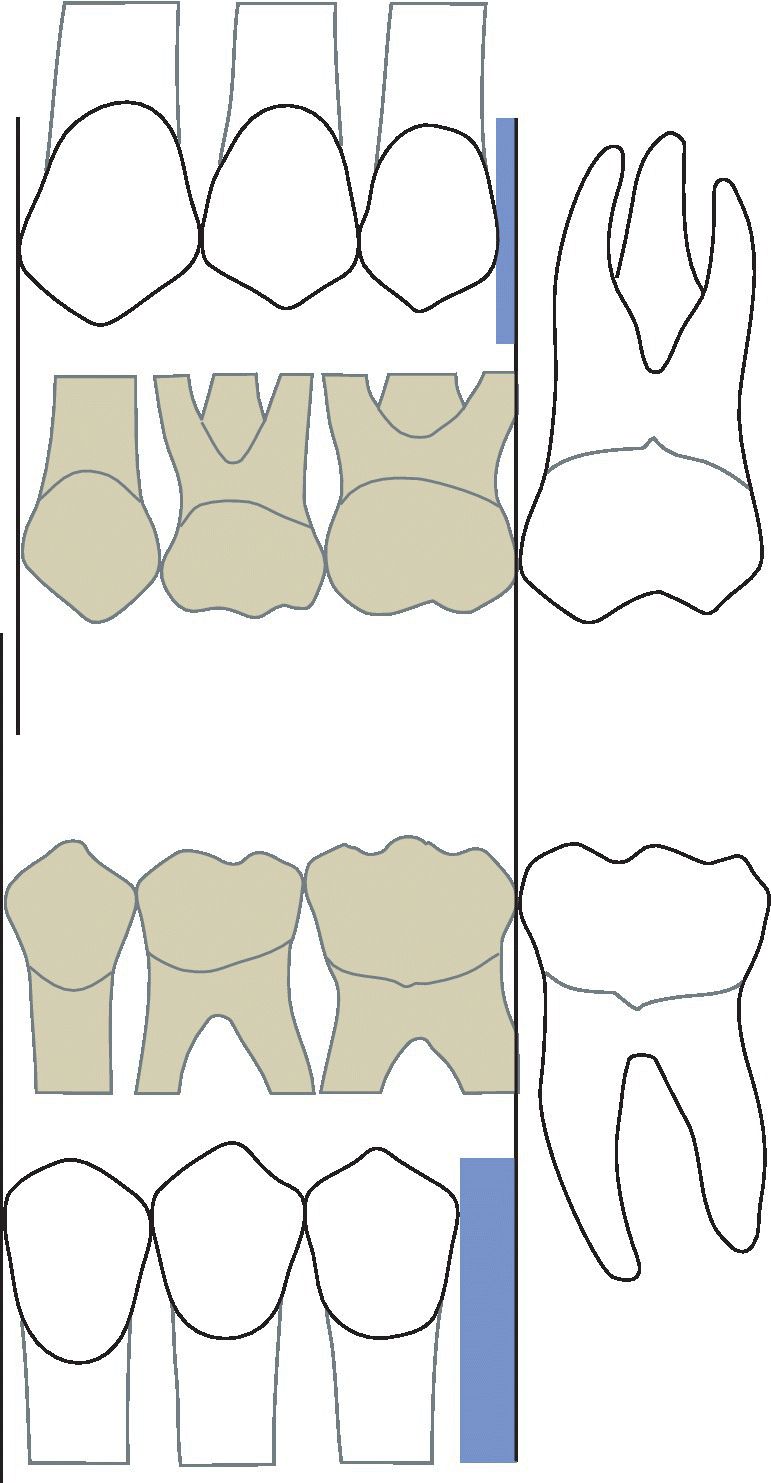
Figure 21.6 The primary canines and molars occupy more space than is necessary for the corresponding group of permanent teeth. The difference is called the “leeway space” and is greater in the mandible (2.5 mm) than in the maxilla (1.5 mm).
Even after completion of the permanent dentition (third molars excluded) the dynamic changes of the dental arches and occlusion continue. On average, the overjet decreases and the dental arches become shorter through mesial drift in the lateral segments, often resulting in a “physiologic” crowding in the lower anterior front of an average of 0.5–1 mm from 12 to 20 years of age. The mean overbite decreases slightly up to the age of 18 years. The transverse dimension of the dental arches, however, tends to remain relatively stable from the early permanent dentition. An increase of palatal height up to adulthood has been reported, thus demonstrating a slow continuous eruption of the teeth. Clinical consequences of that growth will result in an increasing infraposition of ankylosed teeth and implants [4].
Supervising occlusal development in the primary and mixed dentition
In pediatric dentistry the diagnosis and supervision of dental and occlusal development are very important. The responsible dentist should know what to look for in certain developmental stages and also when preventive, interceptive, or corrective measures are indicated and most effective. The eruption of teeth and the developmental status in the jaws may vary by several years within the same age group of individuals. Therefore, a description of dental stages (see Box 7.3) can be made instead of age for describing physiologic maturity. The dental age can be used to estimate the age of children with unknown dates of birth.
Malocclusions
Primary dentition
Etiology
The genetic factors determining the size and position of the jaws are present from conception. Therefore, many of the genetically determined skeletal deviations manifest themselves in the primary dentition. This is especially true for Angle Class II and III, but also for deviations in the transversal dimension, which later are seen as posterior cross bite and scissors bite.
Functional factors such as chewing habits and the chewing resistance of the diet can play a role in the development of malocclusions. This is based on observations of skull materials from people living with primitive feeding habits, and on animal experiments comparing the results of chewing a soft and a hard diet. The evidence is, however, still limited [5,6]. Breathing habits may play a role for facial growth and dental arch morphology. A study reported improvement of open bites and cross bites in young children tonsillectomized because of sleep apnea [7]. It should be remembered, however, that a large proportion of open bites spontaneously correct themselves [8,9].
Habits, mostly dummy and finger sucking, still rank high as etiologic factors for the development of malocclusions in the primary dentition [10] (Box 21.1, Figures 21.7 and 21.8).

Figure 21.7 Posterior cross bite (patient’s left side), midline deviation and mandibular lateral shift, and frontal open bite in a dummy sucker.

Figure 21.8 Results of finger sucking. Asymmetrical left side open bite and overjet.
Prevalence
Malocclusions may be divided into four main groups (Box 21.2):
- deviations in the sagittal plane
- deviations in the vertical plane
- deviations in the transversal plane.
- deviations in available space.
Sagittal plane
Malocclusions in the sagittal plane (Box 21.2) are usually or traditionally measured as deviations in molar relationships and/or size of overjet/negative overjet. However, in the primary dentition we will often find that molar relationships do not give any exact expression for future relations of either jaws or dental arches. Thus, it is more valid to use the canine relations when judging the sagittal relationships in the primary dentition.
Distal molar relationship
Distal molar relations in combination with large overjet is prevalent [11]. In the primary dentition this will be a small problem, but very often this malocclusion will also appear in the permanent dentition. Only in extreme cases where the mandible is held in a distal position, as with a scissors bite or very deep bite, will treatment in the primary dentition be indicated (Figure 21.9).

Figure 21.9 Bilateral scissors bite in combination with forced distal occlusion.
Mesial molar relationship
Mesial molar relations (Angle Class III) with or without negative overjet have a very low prevalence. Negative overjet may exist in neutral molar relation, and we may have mesial molar relation without negative overjet. The malocclusions are divided into three main groups. In reality, most cases present a mixture of skeletal and dentoalveolar deviations:
- skeletal
- dentoalveolar
- functional (forced bite).
In skeletal Class III malocclusions, the size of the maxilla and mandible and/or their positions are disproportional. This may occur in three combinations (Figure 21.10):
- the maxilla is small and/or distally placed
- the mandible is large and/or mesially placed
- a combination of these.
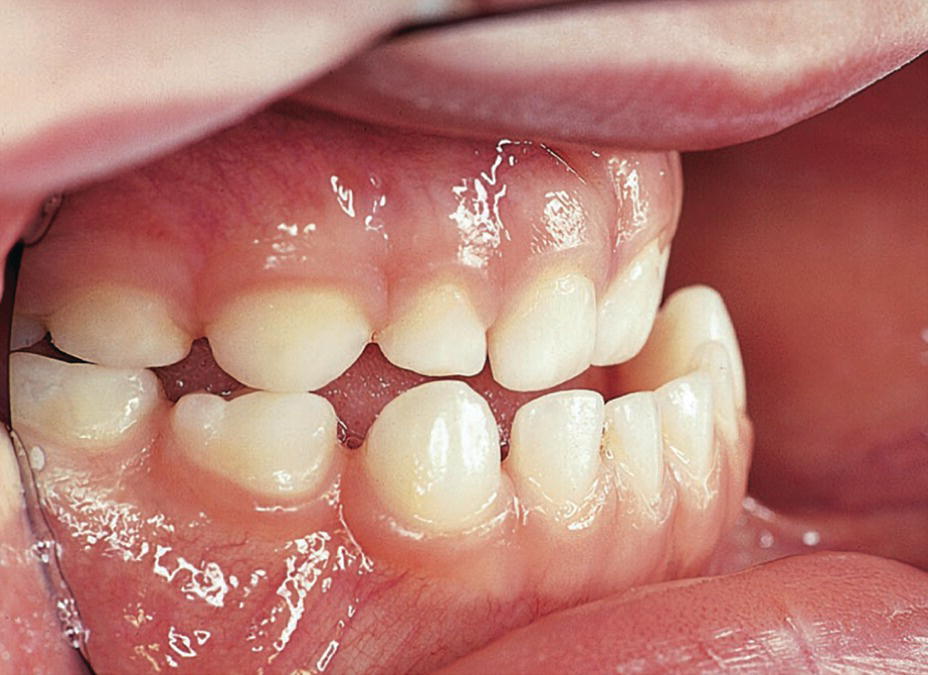
Figure 21.10 Skeletal class III malocclusion without compensation. Note mesial relations between canines.
Whether there will be a normal overjet in the front, an edge‐to‐edge bite, or a negative overjet will depend on the dentoalveolar compensation, which is the degree of labial inclination of incisors in the maxilla and the lingual inclination of the incisors in the mandible.
In cases of dentoalveolar negative overjet there may be a normal relation between the dental arches (best judged on the canine relationship), and the negative overjet is then due to lingual inclination of incisors in the maxilla and labial inclination of incisors in the mandible (Figure 21.11). With forced negative overjet the patient can often bite edge to edge in the retruded contact position of the mandible, but slides forward into negative overjet (pseudo Class III) for full occlusion. The treatment needed for Class III occlusions and anterior cross bite will depend on the severity of the malocclusion and to what extent it causes dissatisfaction for the patient. The dentoalveolar anterior cross bites can usually be left untreated in the primary dentition unless they cause negative effects on space conditions.

Figure 21.11 Dentoalveolar anterior cross bite.
Vertical plane
Malocclusions in the vertical plane (Box 21.2) do not constitute a large problem in the primary dentition. There is a high prevalence of frontal open bite, but it is nearly always dentoalveolar, and often the result of sucking habits. It will most often close when the sucking habit ceases [12,13]. There is also a high prevalence of moderate deep bite, but this has little practical significance unless combined with forced cross bites. Severe deep bite is often combined with overjet and distal occlusion or sometimes scissors bite in lateral segments (Figure 21.12) and will be corrected if these malocclusions are to be treated.

Figure 21.12 Unilateral scissors bite in the primary dentition.
Transversal plane
Malocclusions in the transversal plane (Box 21.2) are dominated by the unilateral forced posterior cross bites; the prevalence is between 10 and 23% [14]. The large range is due to differences in the populations studied, in prevalence of dummy sucking, and also in differences in diagnostic technique. The prevalence of bilateral cross bite and scissors bite is between 3 and 6% [13].
The unilateral forced cross bite is characterized by a narrow, but symmetrical maxilla (Figure 21.13a). In the retruded contact position, the molars will meet cusp‐to‐cusp. To find a stable occlusion, the mandible has to slide to one of the sides, creating a unilateral forced cross bite (Figure 21.13b). The cusps on the cross bite side are often deeply locked into each other, and with little chance of self‐correction (full cross bite) (Figure 21.14). In some patients the maxilla is wider, and the teeth on the cross bite side will meet cusp‐to‐cusp (half cross bite). If the maxilla is very narrow, a bilateral cross bite may be the result. These occlusions are normally not forced and occlude without midline deviation. A bilateral cross bite may be associated with an Angle Class III relation.
Figure 21.13 Forced posterior cross bite. The jaws are symmetrical, but the maxillary jaw is narrow. In the retruded position, the molars occlude cusp‐to‐cusp (a). Full occlusion needs forcing of the bite to the left (b).

Figure 21.14 “Classical” unilateral posterior cross bite. Narrow maxilla with the mandibular midline forced to the cross bite side. Note lack of space in the maxilla.
Cross bites normally establish at eruption of the primary canines and primary second molars. Thus, they may be diagnosed at about 3 years of age. It is important to decide whether the cross bite should be treated in the primary dentition, whether it could be expected to self‐correct, or whether treatment can be postponed until the early mixed dentition (Box 21.3).
VIDEdental - Online dental courses


