2
Deviations in Tooth Morphology and Size
2.1 Introduction
Morphological deviations such as premolarisation of the upper canines,361 maxillary premolars resembling mandibular premolars (Figure 2.1), and lobodontia (“wolf teeth”), that is, enlargement of the middle labial lobe of the canine (Figure 2.2), are rare. Lobodontia may occur together with peg-shaped teeth and multi-cusp molars344 and may also be seen in cases of renal hyperfunction.154 Other morphological deviations are more common.
Figure 2.1 Underdeveloped lingual half (the “deuteromere”) of a maxillary second premolar.
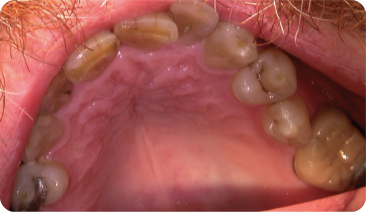
Figure 2.2 Palatal surface of a lobodont maxillary canine (lower panel) and another viewed from labial aspect (upper panel).

2.2 Compression
Compression is when a developing tooth cannot grow to its full size because of being pressed against a hard anatomical barrier.
2.2.1 Appearance and Aetiology
Crown
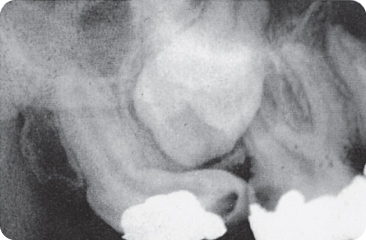
The enamel organ of a compressed maxillary third molar cannot develop to its full size if it is squeezed between the tuberosity and the mineralised crown of the second molar, and the tooth therefore shows an impression of the second molar after mineralisation (Figure 2.3).102 452 Compression of supernumerary teeth102 is rare due to the relative position of the tooth germs in the jaws. However, diagnosis requires a certain degree of caution;102 106 the small, mesio-distally and bucco-palatally elongated, rhomboid crown shapes of the maxillary second molar are not due to compression. Additionally, the canine fossa in the maxillary first premolar, which might guide the erupting canine into its correct place107 is a normal characteristic of these teeth and does not represent compression.
Figure 2.3 (A,B) Compression: a third molar with an underdeveloped mesial aspect due to the already calcified crown of the upper second molar being pressed against the uncalcified mesial side of the third molar during its development. Note the large enamel pearl. (C) The shape of this maxillary second molar crown – broad buccolingually but small mesiodistally – is not a result of compression, but represents the rhomboid crown type.

Root
Factors assumed to cause development of excessively curved roots include anatomical constraints, ectopic location and tooth migration.245 292 402 423 435 Angulation of lower third molar roots has been attributed to idiopathic developmental disturbances510 and to environmental factors and incomplete eruption, which is more prevalent in females.501 The sickle-shaped root (Figure 2.4) is attributed to an eruption path circumventing around scar tissue during root growth. Furthermore, the lack of space and confinement within the hard tissues can supposedly lead to “corkscrew”-shaped roots (Figure 2.5), even in third molars that curve around the second molar during their eruption (Figure 2.6).
Figure 2.4 Sickle-shaped root of a permanent upper incisor.

Figure 2.5 Corkscrew root form of a premolar.

Figure 2.6 Curved root of the third molar as a consequence of erupting around the second molar.
2.2.2 Epidemiology
Currently data on crown compression are scarce. Curved incisor roots are mostly caused by ectopic development,435 but can sometimes represent dilaceration (Section 2.5).423 A small disto-labial curve in the apical half of upper lateral incisor roots is a common occurrence.77 Apical and mid-root curves are seen in 3–4% of (pre)molars.97 In radiographic studies, 15–24% of mandibular third molar and 8–15% of the maxillary molar roots had at least a 90° mesial or distal curvature or a “bull’s eye” appearance, implying a sharp buccal or lingual curvature.179 511
2.3 Dens Invaginatus
Dens invaginatus is a developmental anomaly, a deep invagination of a portion of the enamel organ,493 which results in deeply inverted lingual/occlusal enamel and dentine and often an unusually shaped crown. Other invaginations may originate on the apical and/or lateral tooth surfaces.
The coronally invaginated surface can be described as a deep foramen caecum, the small palatal blind pit that extends deep into the enamel (Figure 2.7). The maxillary lateral incisor is the most commonly affected tooth. The anomaly was (and still is)224 named dens in dente, because radiographs portray an (additional) tooth (germ) embedded in a successor tooth,490 496 636 that is, a “tooth within a tooth”. Alternative names are dilated composite odontome and gestant odontome.
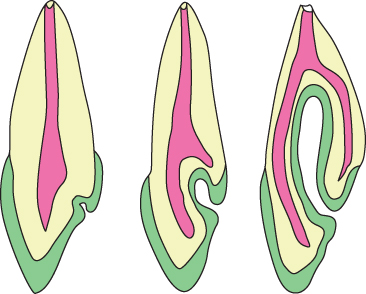
Figure 2.7 Schematic drawings of dens invaginatus: green represents the enamel, yellow the dentine and pink-red the pulp cavity. The left panel shows a lingual foramen caecum. A deepening of the foramen caecum leads to formation of dens invaginatus: if restricted to the crown of the tooth the anomaly is considered to be dens invaginatus type I (middle panel). The right panel illustrates a deep invagination (type II).
Prior to the availability of radiographic diagnostics, the maxillary lateral incisor was thought to be the only tooth affected. Other teeth seldom show this morphological aberration.178 233 337
2.3.1 Coronal
The invagination of the enamel and dentinal tissues creates a small palatal opening, leading to an internal pit lined with enamel.338 The narrow entrance rapidly broadens to form the internal lumen of the invagination.110 Other configurations also exist.
Type I invagination affects the most cervical portion of the tooth. Type II invaginations invade the root portion. Type III invaginations extend into the apex, as if it was a canal with its own apical foramen456 with apical in-growth of cementum. A slightly different classification has also been proposed.176 More than one type of invagination is possible on the same tooth.333 402 Clinically, the crown is often barrel-like or tapers sharply towards the incisal edge,154 338 400 with an unusually broad root.40 193
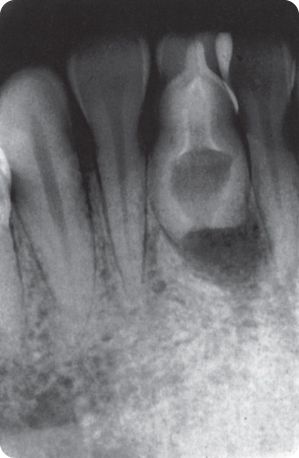
The enamel deep in the invagination is irregular, thin and poorly mineralised319 337 with accessory canal-like channels communicating with the dentine;174 337 392 these probably do not occur in type I invaginations.111 The canals may be restricted to the enamel,40 51 245 but the dentine may also show some patent defects or canals, although such structural irregularities here are few.40 337 The pulp cavity and the lumen of the invagination most likely communicate, but this observation requires histological confirmation.110 359 Figure 2.8 show a maxillary dens invaginatus in situ and the sectioned tooth and Figure 2.9 shows a mandibular invaginated tooth.
Figure 2.8 Dens invaginatus in a permanent maxillary right lateral incisor (A); and the sectioned tooth (B).
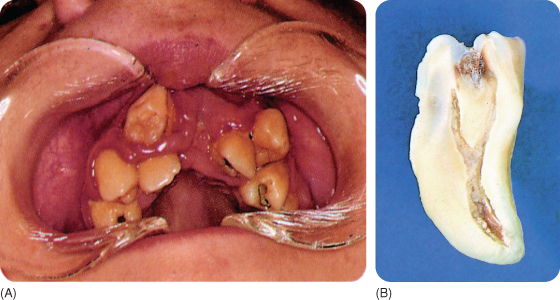
Figure 2.9 Dens invaginatus in the mandible.
Association with Other Anomalies
Dental invaginations are associated with double teeth,115 117 285 288 330 400 the presence of multi-rooted teeth,509 shovel-shaped incisors (Section 2.9.1)235 and the talon (Section 2.10.2);159 339 375 the latter is sometimes referred to as dens evaginatus. Supernumerary teeth, such as the mesiodens,512 may also have invaginations. Conversely, the invaginations may also occur in normal, unaffected teeth in cases of hyperdontia.44 51 213 392 456 Invaginations have been reported in cases of dentinogenesis imperfecta (Chapter 3),232 in taurodontism (Section 2.12), and in cases with increased or decreased numbers of occlusal cusps, microdontia (Section 2.8) and short roots.15 70 208 379 In some instances enamel is grossly lacking.192 Invagination of maxillary lateral incisors is frequently associated with the bilateral presence of Carabelli’s cusp on the maxillary first molars. The occurrence is less frequent with unilateral presence or total absence of the cusp29 (Section 2.10.3). Bilateral dens invaginatus was reported in a young male patient with shovel-shaped incisors, talon and peg-shaped supernumerary incisors.272 It has also been observed in some syndromes (Chapter 11).
2.3.2 Apical
An apical invagination can be considered as the true antipode of the coronal condition.354 The defect is lined with cementum and it has an apical origin.334 The longitudinally orientated, linear invagination has been considered as an anomalous counterpart of the snake’s fang.100
2.3.3 Lateral
The lateral invagination arises in the cervical region of the tooth. It can be seen as a “tube” extending from the cervical crown surface, and is orientated towards the apex, as if it was an extra root canal.85 105 339 401 The lateral invagination can also arise below the cervical area, on the root surface. In both cases the lumen may be lined with enamel, or also with cementum in the case of those that arise below the cervical area.41 A lateral invagination starting below the cervix may also reach high into the crown.424
2.3.4 Epidemiology
Radiographs show that invaginations occur in 0.25–41% of patients.15 24 27 137 167 170 176 177 178 202 205 234 235 259 260 331 352 365 384 395 458 476 The wide variation is largely due to the definition of this anomaly. The foramen caecum, which is present in 30–40% of the population,249 476 should be distinguished from dens invaginatus. To date, arbitrary criteria have been used: (1) The invagination should be deeper than 1 mm176 and (2) the broadened lumen must extend beyond the cingulum.458 The age distribution of the sample may also skew the data due to the fact that many invaginated teeth are extracted early because of aesthetic reasons or pulpal complications. Yet, higher reported percentages seem an overestimation. The prevalence458 of this anomaly may be as low as <0.1% in Western countries, but may be higher elsewhere. The role of familial traits and ethnic background must be recognised in view of the inherited nature of this anomaly.41 170 171 338 379
The coronal type II invagination was by far the most frequently encountered defect in patients referred to one university clinic.375 Some premolars, and in one patient all of them, were invaginated.11 59 178 225 473 Bilateral occurrence is also common,178 375 in approximately 40% of cases.213 Most cases occur in the maxilla, with a few in the mandible;36 159 232 324 343 there is one report of its occurrence concurrently with agenetic incisors.81 Invaginated lower premolars have been reported a few times.30 52 181 225 Invaginated lower canines are very uncommon and an affected primary canine is a rare occurance.162 194 A few deciduous invaginated teeth have been described and on one occasion, a deciduous invaginated molar.122
An invaginated third molar occurring with an ameloblastoma has also been documented.238 Data on the radicular and lateral forms of invagination are scarce.41 195 207 424 These anomalies may occur more often in patients of Chinese or Malaysian descent.339
2.3.5 Aetiology
The development of an invagination requires an infolding of the developing dental hard tissues prior to their calcification. The development of part of the (inner) enamel epithelium might be temporarily arrested or slowed down while the surrounding tissues continue to grow. Theories about focal growth acceleration and/or retardation49 205 206 are merely speculative. Other factors such as localised external pressure fail to explain the occurrence of bilateral dens invaginatus.122
Different inheritance patterns may exist.70 208 In one family, 43% of the parents and 32% of the children were affected.170
2.3.6 Consequences
Caries
The coronal entrance to the invaginated area may be predisposed to plaque accumulation, but surprisingly caries has been diagnosed in only a small proportion of cases.167
Pulpitis
Bacteria colonising the lumen pose a more serious threat to the pulp due to the canal-like defects that exist within the invaginated tissues.381 The frequency of periapical infection has been said not to exceed that in normal incisors,386 but in one study, almost 20% of invaginated teeth had periapical pathology and a further 10% became necrotic despite receiving preventive treatment.375 Pulpitis may ensue not long after the eruption, before the apex has closed.471 Conversely, at 18 years of age, a large proportion of the pulps are still vital;178 this is especially true in type I invagination.111
Periodontal Problems
Bacterial ingress into lateral invaginations that connect the oral cavity with the periodontal tissues leads to (apical) periodontitis.41 85 207 451 456 One invagination located parallel to the root canal, and communicating with the periodontal space at the mid-root, caused a periodontal granuloma; the tooth was treated “endodontically”.168
2.3.7 Prevention of Complications and Treatment
When a visible opening is noted and there is absence of pulpal pathology, sealing this entrance might suffice.206 However, preventive measures often fail due to communicating channels with the pulp cavity, compounded by the fact that tissue present in the lumen of the invagination becomes necrotic post-eruptively. Failure of preventive therapy is not seen in type I invaginations. Preventive cleaning and filling of the lumen of the invagination appears to be the desired therapy, preferably undertaken immediately after eruption. Lining the lumen with calcium hydroxide may lower the chance of pulpal complications.375
The pulp cavity is very complex, with concavities, intracanal communications, inaccessible accessory canals and other anatomical irregularities,111 and may require the complete removal of the invaginated tissues. The anatomy, and root canal(s) openings that are difficult to localise, complicate endodontic treatment, which is not always feasible.49 59 202 383 445 Type II invaginations have been successfully treated with conventional endodontic therapy and apexification, and type III invaginations with surgical root exposure for cleaning and obturation.45 53 111 136 153 159 266 418 450 469 503 Apical curettage or resection may have a favourable outcome438 but success is dependent on many factors. Extraction was the favoured therapy in previous years,205 but this fate – in some cases – may still be inevitable.87
2.4 Palato-Gingival Groove
The palato-gingival groove, a type of invagination, is a sharp, somewhat irregular, funnel-like groove, running from the palatal enamel of the crown and extending along the root. This particularly occurs in the permanent maxillary lateral incisors. Labio-radicular grooves also occur.
2.4.1 Appearance
The groove (Figure 2.10) commonly starts at the junction of the marginal ridge and the cingulum, and then continues along the proximal surface of the root, extending to the apical third of the root251 or to the apex itself. The groove may be visible on radiographs as a narrow radiolucent line.486 Internally, the pulp cavity contour may be altered, with sparse enamel and dentine and increased cementum thickness. Occasionally the pulp cavity may communicate with the periodontal space.251 The groove may be so deep, that a bifurcation and a small, additional proximal root may be present.251 402 Further, the cemento-enamel junction is irregular and distorted in the region of the palatal groove.
Figure 2.10 Lingual groove running from the enamel onto the root.

2.4.2 Epidemiology
Prevalence figures vary from some 2% to 8.5%. The grooves are mainly present in the maxillary lateral incisors.228 239 356 494 Labio-radicular grooves occur mostly in the central incisors and are seldom deep or long. A groove may also be accompanied by dens invaginatus.251 402
2.4.3 Aetiology
The groove results from a superficial infolding of the tooth germ, the cause of which is not known, and parallels the pathogenesis of dens invaginatus, although it is less extensive. Suspected mechanisms include an undesirable location of the lateral incisor germ that is “surrounded” by the central incisor, canine and first premolar.251
2.4.4 Consequences and Treatment
Plaque accumulates subgingivally in the groove, impairing periodontal health and disrupting the gingival attachment.494 Flap reflection, removal of granulation tissue, grinding and flattening of the groove, followed by suturing of a polytetrafluoroethylene (PTFE) membrane has been shown to improve periodontal health.16 Odontoplasty, that is, filling the osseous defects with hydroxyapatite, and additional use of medications (minocycline and chlorhexidine) also resolved the problem.212 In the presence of exposed, patent dentinal tubules or lateral canals, the pulpal tissues may become infected,251 486 possibly creating a combined endodontic-periodontal problem.513 An abnormally shaped pulp canal will hinder endodontic treatment; and failure has been reported.72
2.5 Dilaceration
Dilaceration is a developmental tooth anomaly caused by mechanical trauma that tears away the calcified part of a tooth from the uncalcified part, following which ongoing mineralisation unifies the two parts at an angle to each other.
The dilacerated tooth often shows an abrupt labial change in the axial inclination between the crown and root361 423 (Figures 2.11). The angle should be at least 20°.510 A more apically situated dilaceration results in a tortuously curved root (Figure 2.12). A non-traumatically caused curved or bent root is considered to represent compression (see above).
Figure 2.11 (A) Dilacerated crown of a mandibular permanent lateral incisor; the lingual surface is visible instead of the labial surface. (B) X-ray showing a dilacerated tooth.
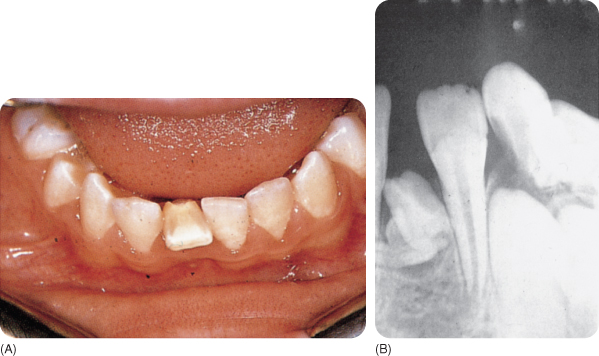
Figure 2.12 Dilacerated root of a lower first premolar.

2.5.1 Aetiology
Mechanical injuries that displace deciduous incisors may damage the tooth germ of the successor teeth, most frequently the maxillary central incisors (Chapter 9). The crown may be partly torn apart from the developing root, but root growth may continue, with deposition of irregular dentine.73 151 278 Traumatic extraction of a primary first molar caused crown dilaceration of the first premolar.294 Direct trauma to an erupting permanent tooth may also cause this deformity.274 Almost 60% of dilacerated teeth show disturbances in amelogenesis484 (Chapter 3).
2.5.2 Prevalence
Among samples of Chinese and Nigerian children, 0.2% had dilacerated, unerupted teeth, assumed to be the consequence of trauma.97 345 Following trauma in the primary dentition, 1% and 3% of the successors had dilacerated roots and crown, respectively.17 18 179 483 In an Iranian sample, 15% had dilacerations.514 Primary teeth are seldom dilacerated.237 Bilateral dilaceration exists.261
2.5.3 Consequences
A dilacerated crown, if erupted, compromises the aesthetics and may show enamel defects (exposing the dentine, which hastens pulpal infection) and a distorted form. Dilacerated roots interfere with endodontic treatment, orthodontics and extraction.
2.5.4 Treatment
When the eruption is delayed, the tooth may be extruded orthodontically after surgical crown exposure.121 264 328 A multidisciplinary approach may be needed295 for cosmetic problems, problems with occlusion and articulation, and possible secondary pathology.
2.6 Enamel Pearls and Enamel Extensions
2.6.1 Enamel Pearls
An enamel pearl is a small oval to round enamel bulb, which may or may not have dentine and pulp tissue. It is typically found on/within the root, and sometimes on the crown. A “true pearl” consists of enamel, a “composite pearl” contains dentine (“enamel-dentine pearl”), and rarely an “enamel-dentine-pulp pearl” may also occur.321 Alternative names are enamel nodules, globules, knots and exostoses. The pearls are often small but some may be up to 4 mm in diameter. They are commonly singular, but two or more pearls may be present on one (primary) tooth.71 248 440
A premolar of a Tibetan sheep was covered with approximately 60 pearls.104 197 A political fugitive took the tooth to India in 1959 and was said to have belonged to a Tibetan saint and presumed to possess protective powers.
Epidemiology
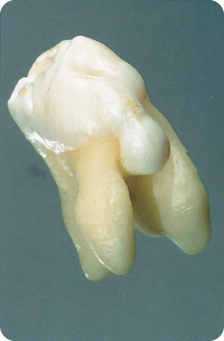
Most pearls are microscopically small and covered with root cementum.320 Larger pearls are obvious on radiographs and after extraction (Figure 2.13).
Figure 2.13 Enamel pearl.

Of 2000 extracted teeth, 2.5% showed enamel pearls, a few embedded in the root and one in the crown.71 In a radiographic study, pearls were present in about 5% of patients.95 Macroscopically visible pearls were present on 1.6% of teeth, the majority of which were in the cervical area of the maxillary molars, especially distally. A stereo-microscopic study found enamel islets on 5% and enamel “drops” on 1.6% of multi-rooted teeth.440 Enamel islets are exclusively located along the inter-radicular grooves, especially buccally and distally, and in the furcations.440
Considerably higher prevalence rates of enamel pearls have also been reported.158 In a microradiographic study, enamel pearls were found in the furcation of one-third of deciduous molars.21 In nine surveys, the mean prevalence was 2.7%.321 They seem more common in people of Inuit decent (about 10%) than in other races.321 361
Histology
There are three types of enamel pearl: (1) pearls within the dentine that originate at the time of the dentinogenesis, (2) pearls on the root surface, which affect dentine formation, and (3) pearls on the root surface that do not affect dentinogenesis and easily break away.71 The enamel structure is disorganised, but the chemical composition is normal,21 377 although the enamel prisms running parallel to the surface are hypocalcified.231 In contrast to larger pearls, small ones have a high content of residual enamel matrix and a low mineral content.47 Hunter–Schreger bands are rarely visible and the striae of Retzius are irregular (Chapter 3). Pulp tissue forming in the pearls communicates with the main pulpal tissue.231
Aetiology
The cause and pathogenesis are uncertain. Hertwig’s root sheath is suggested to preserve or recover local potential for cell proliferation and differentiation103 321 and produce the enamel pearls. Amelogenins found in the dentinal tubules adjacent to the pearls suggest diffusion of the proteins towards the pulp,47 but enamel protein synthesis by pulpal cells of mesenchymal origin seems possible too.134
The network of epithelial remnants (named after Malassez) of Hertwig’s sheath could produce the pearls, but Malassez rejected this idea.321 Perforation of the radicular pulp in young rats has been seen to cause migration of the root epithelium, which produced structures resembling the Malassez epithelial remnants. In contact with calcified osteodentine, the remnants in the pulp transformed into ameloblast-like cells that secreted amelogenin.177 Secretory ameloblasts express over 1000 times the level of amelogenin mRNA than odontoblasts.342
Although beyond the scope of this book, cementum pearls are anomalies on the maturing enamel of continuously erupting guinea pig molars.210 Enamel pearls should not be confused on basis of their name with Epstein pearls, which are keratin-filled cysts that occur in the mid-palatine raphe region close to the mucosal surface in about 80% of neonates. The cysts usually resolve within a few months.188
Consequences and Treatment
Larger pearls may interfere with the removal of calculus and there is a risk of fracture of the tip of the scaler. Small pearls may show up on radiographs, resembling calculus.412 Unless the pearls are associated with localised periodontal destruction,86 155 321 422 treatment is not required.
2.6.2 Enamel Extensions
An enamel extension is enamel running from the cervical region of the crown towards or into the furcation area of molars. Class III extensions reach the root furcation proper (Figure 2.14), class II run halfway, and class I are less deep.293 Class III has been subdivided into IIIa, a long slender enamel projection into the furcation, and IIIb, an interrupted or discontinued projection.506 The extensions may end in an enamel bulge (Figure 2.15), which might be considered a separate type.401
Figure 2.14 Cervical enamel extension.

Figure 2.15 Enamel projection with a thick spherical end.
Epidemiology
The extensions occur particularly on the buccal side190 507 in 8.3–33.6% of cases in different populations.43 171 172 256 293 376 440 442 466 507 Mandibular second molars are particularly affected. In Asian populations, 40–78% molars have enamel projections, as do two-thirds in the Inuit population.506 Observational studies including magnified examination (×15) show that the majority of molars possess enamel extensions. The occurrence of enamel pearls and extensions concurrently has been reported.196 In some studies, class III extensions represented a large minority of the cases with extentions.171 257 293 An extension on a maxillary incisor was reported to emerged through the overlying gingiva.22
Aetiology
The cause is either bulging out of the enamel organ or the Hertwig’s sheath together with the inner and outer epithelium, the stratum intermedium and reticulum stellare, creating locally favourable conditions for amelogenesis.
Consequences
The gingiva cannot attach to the enamel and the extensions allow dental plaque to accumulate subgingivally, predisposing to periodontal disease. This may happen near or within the root furcation.43 171 198 199 281 442 Not all researchers report extensions related to pocket formation.256 Presence of extensions is reported in 22% of periodontal furcation problems.43 In a group of molars, 60% had furcation problems,488 of which more than 80% possessed extensions, generally long ones.199 281 Pearl-like extensions encouraging local plaque stagnation can be removed after raising a flap.
2.7 Fused Roots
Fused roots occur when, in principle, multi-rooted teeth share part of their root dentine. Here, root grooves essentially indicate that more roots exist and several root canals are present.
2.7.1 Aetiology
Either incomplete invaginations of Hertwig’s sheath4 or lack of space are said to underlie roo/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


